

A descriptive study of the clinical and etiological profile of balanoposthitis
- PMID: 34322423
- PMCID: PMC8284224
- DOI: 10.4103/jfmpc.jfmpc_2467_20
A descriptive study of the clinical and etiological profile of balanoposthitis
Abstract
Background: Balanoposthitis is defined as an inflammatory condition of glans penis and prepuce. There are wide variety of etiologies including both infectious and noninfectious conditions. This study attempts to throw light on information regarding clinical and microbiological aspects of balanoposthitis.
Objectives: To study various clinical patterns, etiologies, and predisposing factors of balanoposthitis.
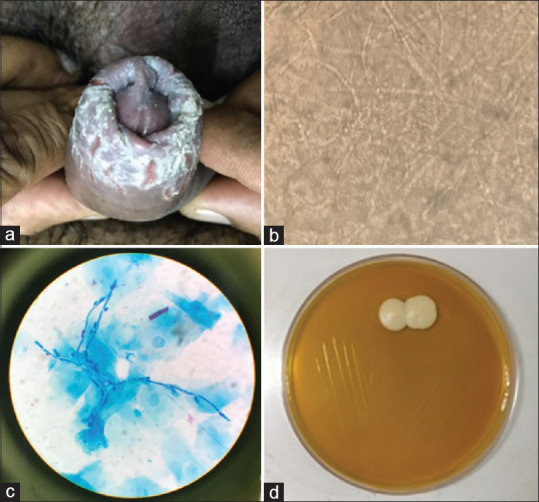
Methodology: A descriptive study was undertaken on 106 cases who presented to sexually transmitted disease (STD) clinic with balanoposthitis between November 2017 and April 2019. A detailed history, physical examination, and investigations like KOH mount, leishman staining, gram staining, dark field microscopy, cultures, and other investigations were done wherever indicated. The data collected was tabulated and analyzed.
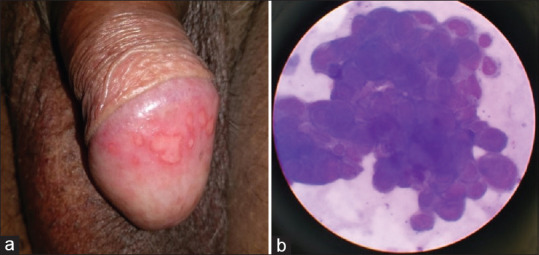
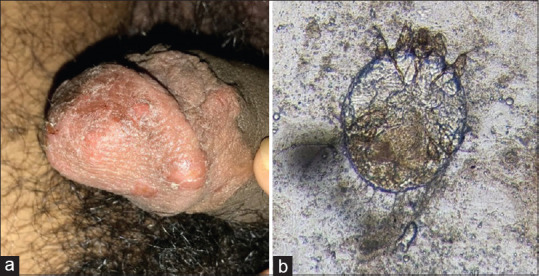
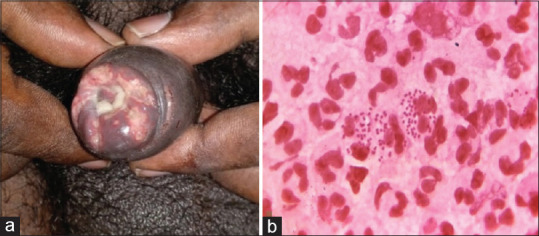
Results: In our study, infectious etiology was the most common and was found in 77.36% cases. About 13.41% of cases with infectious balanoposthitis had multiple etiological agents. Noninfectious etiology was found in 22.64% cases. The most common infectious cause of balanoposthitis was candida, noted in 59.76% cases, followed by herpes simplex virus (19.51%), human papilloma virus (13.41%), and scabies (8.54%). Among noninfectious etiologies, adverse drug reaction (4.72% of total cases) was the most common, followed by lichen planus (3.77%) and psoriasis (3.77%). There was significantly higher incidence of phimosis in diabetic patients with candidal balanoposthitis.
Conclusion: Identifying the etiology facilitates early treatment and hence reduces the infectivity and transmission of disease and also the disease complications like phimosis. In addition, multiple infectious etiologies should always be kept in mind while evaluating STDs.
Keywords: Balanoposthitis; candidal; genital warts; herpes genitalis.
Copyright: © 2021 Journal of Family Medicine and Primary Care.
Conflict of interest statement
There are no conflicts of interest.
Figures


Similar articles
-
Morphological Patterns of Balanoposthitis and their Correlation with Final Etiological Diagnosis.Indian Dermatol Online J. 2023 Feb 23;14(2):187-194. doi: 10.4103/idoj.idoj_197_22. eCollection 2023 Mar-Apr. Indian Dermatol Online J. 2023. PMID: 37089850 Free PMC article.
-
Sexual Dysfunction Evaluation in Candidal Balanoposthitis: A Single Centred Observational Study.J Family Reprod Health. 2023 Mar;17(1):8-13. doi: 10.18502/jfrh.v17i1.11971. J Family Reprod Health. 2023. PMID: 37538229 Free PMC article.
-
Balanoposthitis.2024 May 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 May 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31971711 Free Books & Documents.
-
Common skin disorders of the penis.BJU Int. 2002 Sep;90(5):498-506. doi: 10.1046/j.1464-410x.2002.02962.x. BJU Int. 2002. PMID: 12175386 Review.
-
[Balanoposthitis in the clinical practice of a urologist and dermatovenereologist: an interdisciplinary problem].Urologiia. 2023 Dec;(6):152-157. Urologiia. 2023. PMID: 38156700 Review. Russian.
Cited by
-
Morphological Patterns of Balanoposthitis and their Correlation with Final Etiological Diagnosis.Indian Dermatol Online J. 2023 Feb 23;14(2):187-194. doi: 10.4103/idoj.idoj_197_22. eCollection 2023 Mar-Apr. Indian Dermatol Online J. 2023. PMID: 37089850 Free PMC article.
-
Computer-assisted sperm analysis of the epididymal spermatozoa in dromedary camels suffering from penile and preputial pathological problems.Front Vet Sci. 2025 Mar 14;12:1537708. doi: 10.3389/fvets.2025.1537708. eCollection 2025. Front Vet Sci. 2025. PMID: 40160704 Free PMC article.
-
Etiology, clinical manifestations, and management methods of cryptitis beside the preputial frenulum in men.Basic Clin Androl. 2024 Jan 16;34(1):3. doi: 10.1186/s12610-024-00219-0. Basic Clin Androl. 2024. PMID: 38229107 Free PMC article.
-
Chinese expert consensus on the diagnosis and treatment of balanoposthitis.Chin Med J (Engl). 2024 Jul 5;137(13):1519-1521. doi: 10.1097/CM9.0000000000003172. Epub 2024 Jun 11. Chin Med J (Engl). 2024. PMID: 38863122 Free PMC article. No abstract available.
References
-
- Cuckow PM. FORESKIN [Internet]. Pediatric Urology. 2nd ed. W. B. Saunders; 2009.
-
- Lisboa C, Ferreira A, Resende C, Rodrigues AG. Infectious balanoposthitis: Management, clinical and laboratory features. Int J Dermatol. 2009;48:121–4. - PubMed
-
- Raju J, Prakash BG. Balanoposthitis: A clinical study. J Evid Based Med Healthcare. 2015;2:249–60.
-
- Lisboa c, Santos A, Dias C, Azevedo F, Pina-Vaz C, Rodrigues A. Candida balanitis: Risk factors. J Eur Acad Dermatol Venereol. 2010;24:820–6. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous