

Disparities in Emergency Medical Services Time Intervals for Patients with Suspected Acute Coronary Syndrome: Findings from the North Carolina Prehospital Medical Information System
- PMID: 34323113
- PMCID: PMC8475668
- DOI: 10.1161/JAHA.120.019305
Disparities in Emergency Medical Services Time Intervals for Patients with Suspected Acute Coronary Syndrome: Findings from the North Carolina Prehospital Medical Information System
Abstract
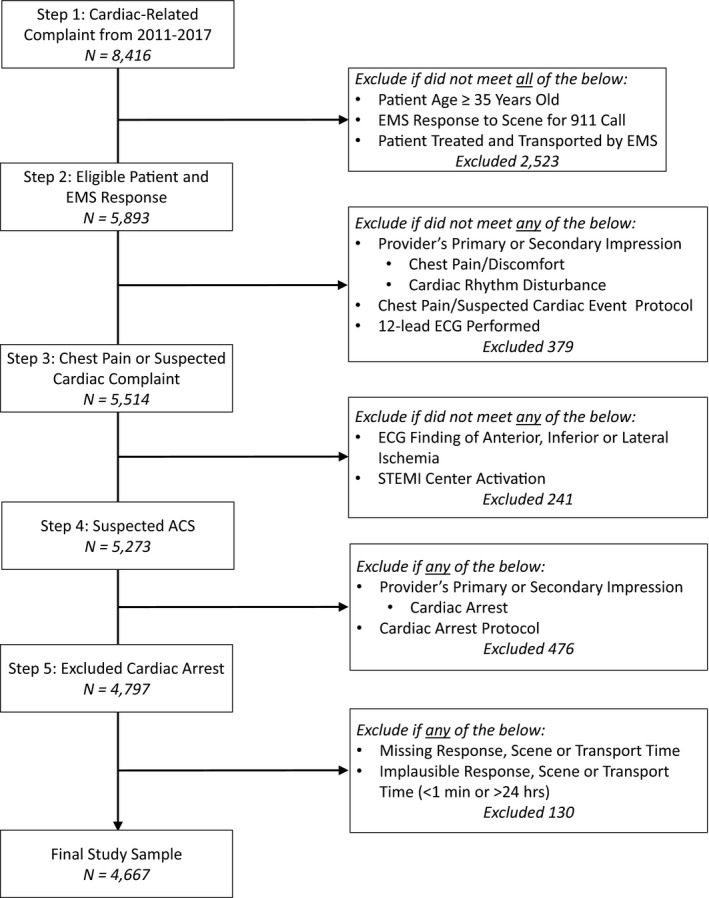
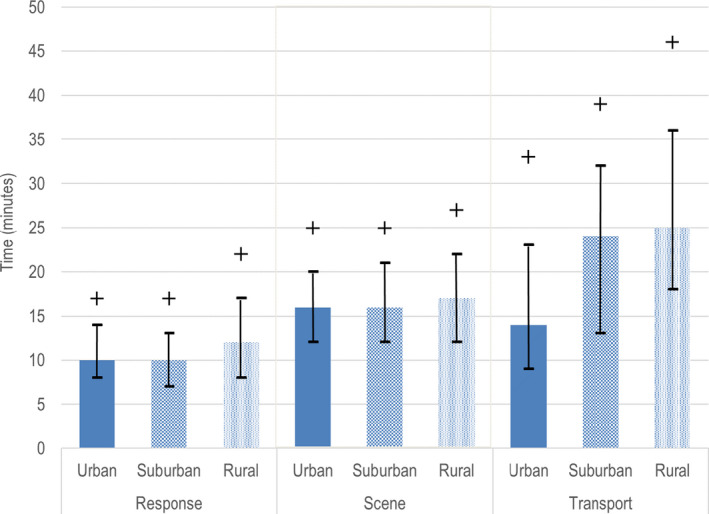
Background Timely emergency medical services (EMS) response, management, and transport of patients with suspected acute coronary syndrome (ACS) significantly reduce delays to emergency treatment and improve outcomes. We evaluated EMS response, scene, and transport times and adherence to proposed time benchmarks for patients with suspected ACS in North Carolina from 2011 to 2017. Methods and Results We conducted a population-based, retrospective study with the North Carolina Prehospital Medical Information System, a statewide electronic database of all EMS patient care reports. We analyzed 2011 to 2017 data on patient demographics, incident characteristics, EMS care, and county population density for EMS-suspected patients with ACS, defined as a complaint of chest pain or suspected cardiac event and documentation of myocardial ischemia on prehospital ECG or prehospital activation of the cardiac care team. Descriptive statistics for each EMS time interval were computed. Multivariable logistic regression was used to quantify relationships between meeting response and scene time benchmarks (11 and 15 minutes, respectively) and prespecified covariates. Among 4667 patients meeting eligibility criteria, median response time (8 minutes) was shorter than median scene (16 minutes) and transport (17 minutes) time. While scene times were comparable by population density, patients in rural (versus urban) counties experienced longer response and transport times. Overall, 62% of EMS encounters met the 11-minute response time benchmark and 49% met the 15-minute scene time benchmark. In adjusted regression analyses, EMS encounters of older and female patients and obtaining a 12-lead ECG and venous access were independently associated with lower adherence to the scene time benchmark. Conclusions Our statewide study identified urban-rural differences in response and transport times for suspected ACS as well as patient demographic and EMS care characteristics related to lower adherence to scene time benchmark. Strategies to reduce EMS scene times among patients with ACS need to be developed and evaluated.
Keywords: acute coronary syndrome; disparities; emergency medical services; prehospital delay.
Conflict of interest statement
None.
Figures
References
-
- Huynh T, Perron S, O'Loughlin J, Joseph L, Labrecque M, Tu JV, Théroux P. Comparison of primary percutaneous coronary intervention and fibrinolytic therapy in ST‐segment–elevation myocardial infarction: bayesian hierarchical meta‐analyses of randomized controlled trials and observational studies. Circulation. 2009;119:3101–3109. DOI: 10.1161/CIRCULATIONAHA.108.793745. - DOI - PubMed
-
- Nallamothu BK, Normand SL, Wang Y, Hofer TP, Brush JE Jr, Messenger JC, Bradley EH, Rumsfeld JS, Krumholz HM. Relation between door‐to‐balloon times and mortality after primary percutaneous coronary intervention over time: a retrospective study. Lancet. 2015;385:1114–1122. DOI: 10.1016/S0140-6736(14)61932-2. - DOI - PMC - PubMed
-
- Scholz KH, Maier SKG, Maier LS, Lengenfelder B, Jacobshagen C, Jung J, Fleischmann C, Werner GS, Olbrich HG, Ott R, et al. Impact of treatment delay on mortality in ST‐segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT‐STEMI trial. Eur Heart J. 2018;39:1065–1074. DOI: 10.1093/eurheartj/ehy004. - DOI - PMC - PubMed
-
- Nepper‐Christensen L, Lønborg J, Høfsten DE, Ahtarovski KA, Kyhl K, Göransson C, Køber L, Helqvist S, Pedersen F, Kelbæk H, et al. Impact of diagnostic ECG‐to‐wire delay in STEMI patients treated with primary PCI: a DANAMI‐3 substudy. EuroIntervention. 2018;14:700–707. DOI: 10.4244/EIJ-D-17-00857. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
