

Reducing Cardiovascular Maternal Mortality by Extending Medicaid for Postpartum Women
- PMID: 34323114
- PMCID: PMC8475675
- DOI: 10.1161/JAHA.121.022040
Reducing Cardiovascular Maternal Mortality by Extending Medicaid for Postpartum Women
Abstract
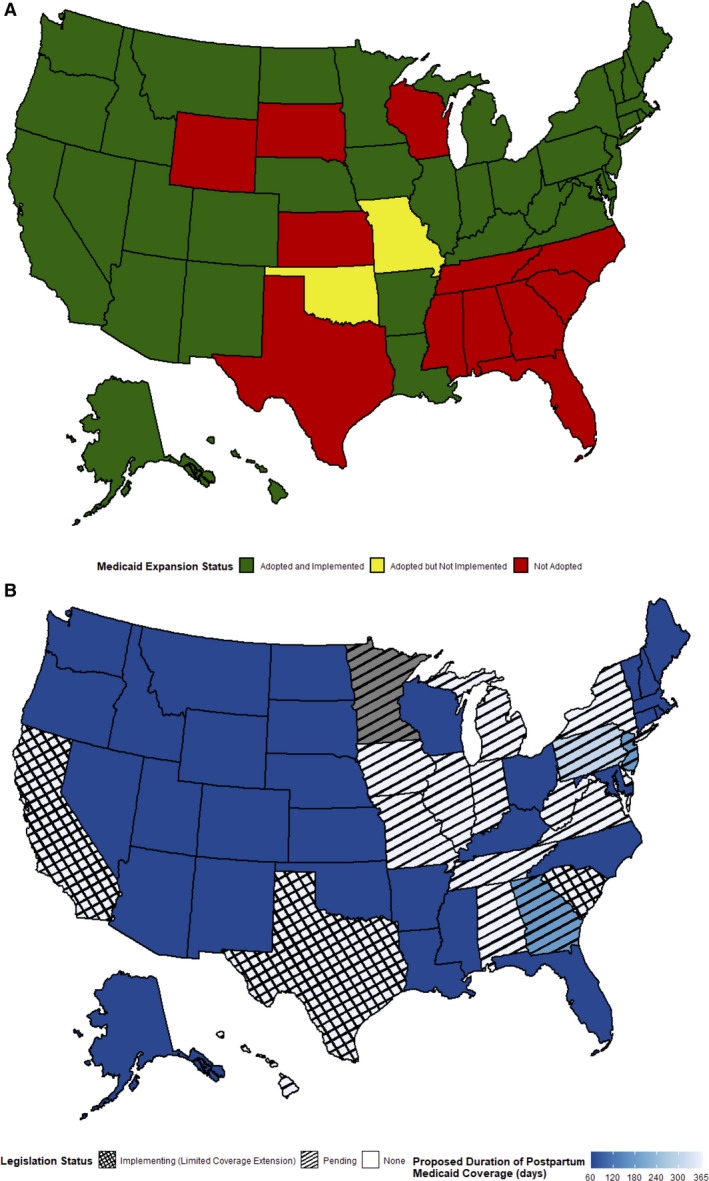
Maternal mortality has been increasing in the United States over the past 3 decades, while decreasing in all other high-income countries during the same period. Cardiovascular conditions account for over one fourth of maternal deaths, with two thirds of deaths occurring in the postpartum period. There are also significant healthcare disparities that have been identified in women experiencing maternal morbidity and mortality, with Black women at 3 to 4 times the risk of death as their White counterparts and women in rural areas at heightened risk for cardiovascular morbidity and maternal morbidity. However, many maternal deaths have been shown to be preventable, and improving access to care may be a key solution to addressing maternal cardiovascular mortality. Medicaid currently finances almost half of all births in the United States and is mandated to provide coverage for women with incomes up to 138% of the federal poverty level, for up to 60 days postpartum. In states that have not expanded coverage, new mothers become uninsured after 60 days. Medicaid expansion has been shown to reduce maternal mortality, particularly benefiting racial and ethnic minorities, likely through reduced insurance churn, improved postpartum access to care, and improved interpregnancy care. However, even among states with Medicaid expansion, significant care gaps exist. An additional proposed intervention to improve access to care in these high-risk populations is extension of Medicaid coverage for 1 year after delivery, which would provide the most benefit to women in Medicaid nonexpanded states, but also improve care to women in Medicaid expanded states.
Keywords: Medicaid; health policy; postpartum.
Conflict of interest statement
Dr Joynt Maddox receives research support from the National Heart, Lung, and Blood Institute (R01HL143421) and National Institute on Aging (R01AG060935, R01AG063759, and R21AG065526), and previously did contract work for the US Department of Health and Human Services. The remaining authors have no disclosures to report.
Figures

Similar articles
-
Expand and extend postpartum Medicaid to support maternal and child health.Transl Behav Med. 2024 Apr 29;14(5):298-300. doi: 10.1093/tbm/ibae007. Transl Behav Med. 2024. PMID: 38417096
-
Association of Expanded Prenatal Care Coverage for Immigrant Women With Postpartum Contraception and Short Interpregnancy Interval Births.JAMA Netw Open. 2021 Aug 2;4(8):e2118912. doi: 10.1001/jamanetworkopen.2021.18912. JAMA Netw Open. 2021. PMID: 34338791 Free PMC article.
-
Racial and ethnic disparities in postpartum care and contraception in California's Medicaid program.Am J Obstet Gynecol. 2017 Jul;217(1):47.e1-47.e7. doi: 10.1016/j.ajog.2017.02.040. Epub 2017 Mar 3. Am J Obstet Gynecol. 2017. PMID: 28263752
-
Medicaid and moms: the potential impact of extending medicaid coverage to mothers for 1 year after delivery.J Perinatol. 2022 Jun;42(6):819-824. doi: 10.1038/s41372-021-01299-w. Epub 2022 Feb 7. J Perinatol. 2022. PMID: 35132151 Review.
-
The ACA Medicaid Expansion And Perinatal Insurance, Health Care Use, And Health Outcomes: A Systematic Review.Health Aff (Millwood). 2022 Jan;41(1):60-68. doi: 10.1377/hlthaff.2021.01150. Health Aff (Millwood). 2022. PMID: 34982621
Cited by
-
Postpartum Medicaid coverage and outpatient care utilization among low-income birthing individuals in Oregon: impact of Medicaid expansion.Front Public Health. 2023 Jul 4;11:1025399. doi: 10.3389/fpubh.2023.1025399. eCollection 2023. Front Public Health. 2023. PMID: 37469686 Free PMC article.
-
Racial/Ethnic Disparities in Postpartum Health Insurance Coverage Among Rural and Urban U.S. Residents.J Womens Health (Larchmt). 2022 Oct;31(10):1397-1402. doi: 10.1089/jwh.2022.0169. Epub 2022 Aug 30. J Womens Health (Larchmt). 2022. PMID: 36040353 Free PMC article.
-
Women's Health: Population Patterns and Social Determinants.Annu Rev Sociol. 2022 Jul;48:277-298. doi: 10.1146/annurev-soc-030320-034200. Epub 2022 May 13. Annu Rev Sociol. 2022. PMID: 38765764 Free PMC article.
-
Can We Implement Multispecialty Mother-Infant Dyadic Care to Systematize Interpregnancy Services After a Preterm Birth?Womens Health Rep (New Rochelle). 2023 Dec 18;4(1):651-655. doi: 10.1089/whr.2023.0148. eCollection 2023. Womens Health Rep (New Rochelle). 2023. PMID: 38155872 Free PMC article. No abstract available.
-
Functional Adaptations in Coronary Reactivity following Healthy Pregnancy in Swine.J Vasc Res. 2025;62(2):78-87. doi: 10.1159/000543116. Epub 2024 Dec 11. J Vasc Res. 2025. PMID: 39662079
References
-
- Centers for Disease Control (CDC) . Pregnancy mortality surveillance system. https://www.cdc.gov/reproductivehealth/maternal‐mortality/pregnancy‐mort.... Accessed May 27, 2020.
-
- Centers for Disease Control (CDC) . Report from nine maternal mortality review committees. https://www.cdcfoundation.org/sites/default/files/files/ReportfromNineMM.... Accessed October 22, 2020.
-
- Centers for Disease Control (CDC) . Pregnancy‐related deaths: data from 14 U.S. maternal mortality review committees, 2008–2017. https://www.cdc.gov/reproductivehealth/maternal‐mortality/erase‐mm/mmr‐d.... Accessed October 22, 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
