

Pharmacokinetics and Safety of 3 Months of Weekly Rifapentine and Isoniazid for Tuberculosis Prevention in Pregnant Women
- PMID: 34323955
- PMCID: PMC9070820
- DOI: 10.1093/cid/ciab665
Pharmacokinetics and Safety of 3 Months of Weekly Rifapentine and Isoniazid for Tuberculosis Prevention in Pregnant Women
Abstract
Background: Pregnancy increases the risk of tuberculosis and its complications. A 3-month regimen of weekly isoniazid and rifapentine (3HP) is safe and effective for tuberculosis prevention in adults and children, including those with HIV, but 3HP has not been evaluated in pregnancy.
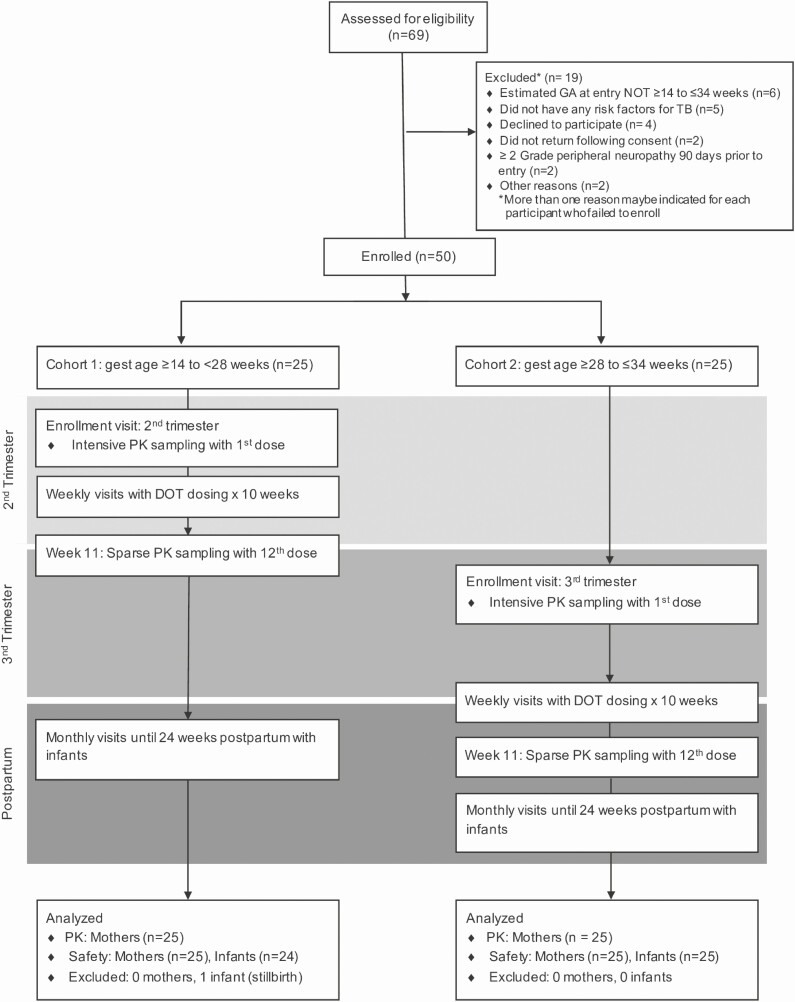
Methods: IMPAACT 2001 was a phase I/II trial evaluating the pharmacokinetics and safety of 3HP among pregnant women with indications for tuberculosis preventative therapy in Haiti, Kenya, Malawi, Thailand, and Zimbabwe (NCT02651259). Isoniazid and rifapentine were provided at standard doses (900 mg/week). Pharmacokinetic sampling was performed with the first (second/third trimester) and twelfth (third trimester/postpartum) doses. Nonlinear mixed-effects models were used to estimate drug population pharmacokinetics.
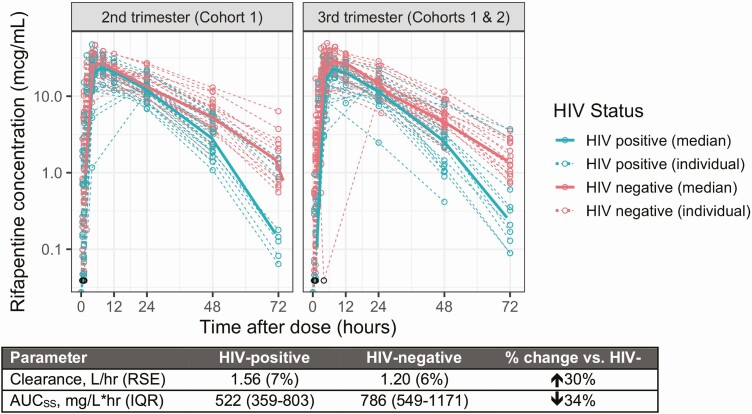
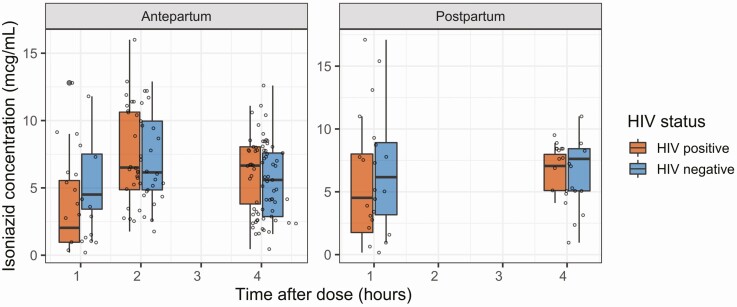
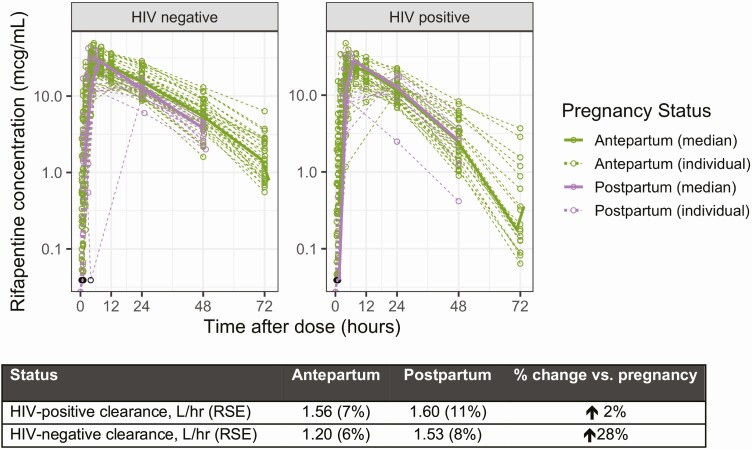
Results: Of 50 participants, 20 had HIV and were taking efavirenz-based antiretroviral therapy. Among women without HIV, clearance of rifapentine was 28% lower during pregnancy than postpartum (1.20 vs 1.53 L/hour, P < .001), with area under the concentration-time curve (AUCSS) of 786 and 673 mg × hour/L, respectively. In pregnant women with HIV, clearance was 30% higher than women without HIV (P < .001), resulting in lower AUCss (522 mg × hour/L); clearance did not change significantly between pregnancy and postpartum. Pregnancy did not impact isoniazid pharmacokinetics. There were no drug-related serious adverse events, treatment discontinuations, or tuberculosis cases in women or infants.
Conclusions: 3HP does not require dose adjustment in pregnancy. Rifapentine clearance is higher among women with HIV, but all women achieved exposures of rifapentine and isoniazid associated with successful tuberculosis prevention. The data support proceeding with larger safety-focused studies of 3HP in pregnancy.
Clinical trials registration: ClinicalTrials.gov, NCT02651259.
Keywords: HIV; latent tuberculosis; maternal health; pharmacokinetics; rifapentine.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Zenner D, Kruijshaar ME, Andrews N, Abubakar I. Risk of tuberculosis in pregnancy: A national, primary care-based cohort and self-controlled case series study. Am J Respir Crit Care Med 2012; 185:779–84. Available at: http://www.atsjournals.org/doi/abs/10.1164/rccm.201106-1083OC. Accessed 22 July 2020. - DOI - PubMed
-
- Sugarman J, Colvin C, Moran AC, Oxlade O. Tuberculosis in pregnancy: An estimate of the global burden of disease. Lancet Glob Heal 2014; 2:e710–6. Available at: https://pubmed.ncbi.nlm.nih.gov/25433626/. Accessed 28 June 2021. - PubMed
-
- Say L, Chou D, Gemmill A, et al. . Global causes of maternal death: A WHO systematic analysis. Lancet Glob Heal 2014; 2:e323–33. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI068632/AI/NIAID NIH HHS/United States
- Z01 AI000686/ImNIH/Intramural NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- UM1 AI106716/AI/NIAID NIH HHS/United States
- K24 AI150349/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- K23 AI129854/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- HHSN275201800001I/HD/NICHD NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
