

Socioeconomic variation in characteristics, outcomes, and healthcare utilization of COVID-19 patients in New York City
- PMID: 34324574
- PMCID: PMC8321227
- DOI: 10.1371/journal.pone.0255171
Socioeconomic variation in characteristics, outcomes, and healthcare utilization of COVID-19 patients in New York City
Abstract
Objectives: There is limited evidence on how clinical outcomes differ by socioeconomic conditions among patients with coronavirus disease 2019 (COVID-19). Most studies focused on COVID-19 patients from a single hospital. Results based on patients from multiple health systems have not been reported. The objective of this study is to examine variation in patient characteristics, outcomes, and healthcare utilization by neighborhood social conditions among COVID-19 patients.
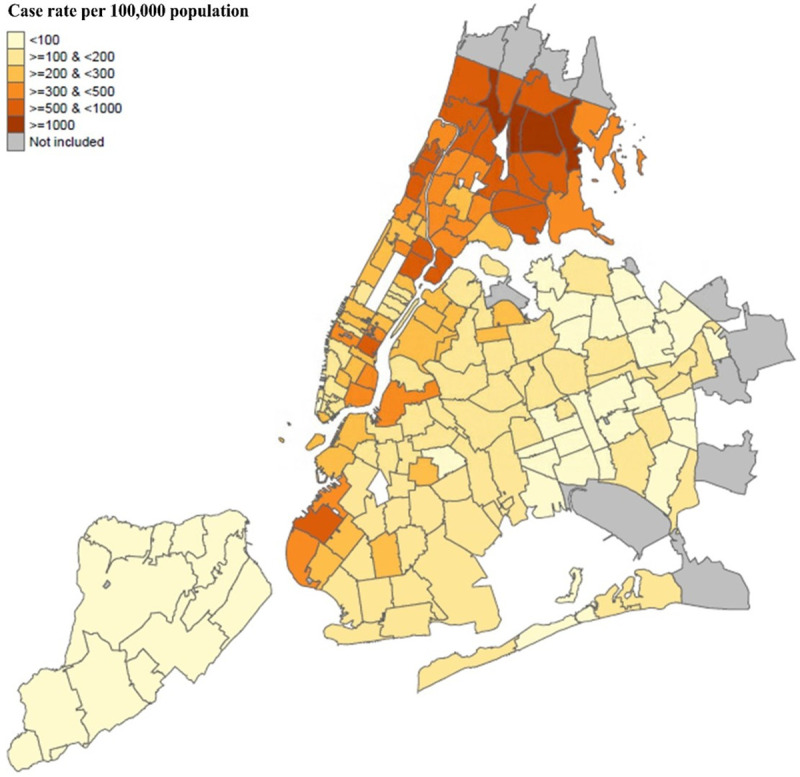
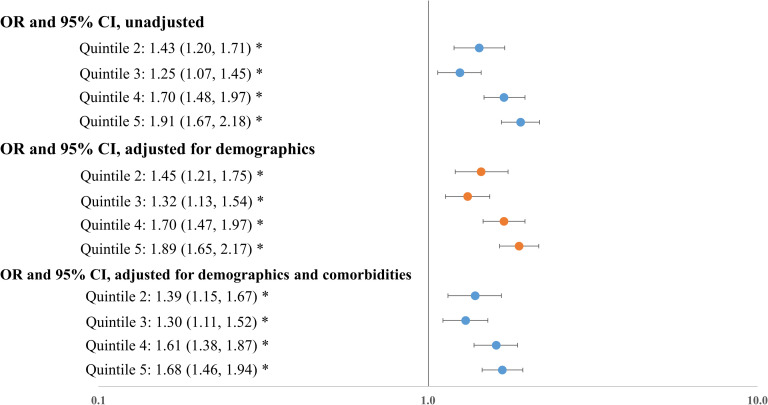
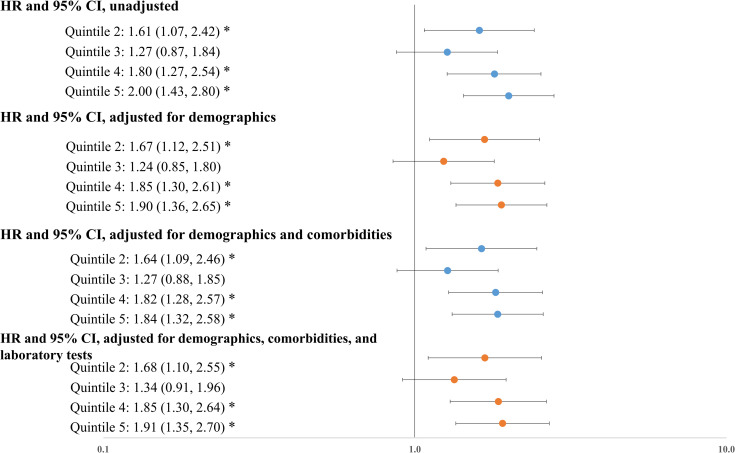
Methods: We extracted electronic health record data for 23,300 community dwelling COVID-19 patients in New York City between March 1st and June 11th, 2020 from all care settings, including hospitalized patients, patients who presented to the emergency department without hospitalization, and patients with ambulatory visits only. Zip Code Tabulation Area-level social conditions were measured by the Social Deprivation Index (SDI). Using logistic regressions and Cox proportional-hazards models, we examined the association between SDI quintiles and hospitalization and death, controlling for race, ethnicity, and other patient characteristics.
Results: Among 23,300 community dwelling COVID-19 patients, 60.7% were from neighborhoods with disadvantaged social conditions (top SDI quintile), although these neighborhoods only account for 34% of overall population. Compared to socially advantaged patients (bottom SDI quintile), socially disadvantaged patients (top SDI quintile) were older (median age 55 vs. 53, P<0.001), more likely to be black (23.1% vs. 6.4%, P<0.001) or Hispanic (25.4% vs. 8.5%, P<0.001), and more likely to have chronic conditions (e.g., diabetes: 21.9% vs. 10.5%, P<0.001). Logistic and Cox regressions showed that patients with disadvantaged social conditions had higher risk for hospitalization (odds ratio: 1.68; 95% confidence interval [CI]: [1.46, 1.94]; P<0.001) and mortality (hazard ratio: 1.91; 95% CI: [1.35, 2.70]; P<0.001), adjusting for other patient characteristics.
Conclusion: Substantial socioeconomic disparities in health outcomes exist among COVID-19 patients in NYC. Disadvantaged neighborhood social conditions were associated with higher risk for hospitalization, severity of disease, and death.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- NYC Health. COVID-19: Data 2020 [cited 2021 06/20]. Available from: https://www1.nyc.gov/site/doh/covid/covid-19-data.page.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
