

Safety, tolerability, and immunogenicity of an aerosolised adenovirus type-5 vector-based COVID-19 vaccine (Ad5-nCoV) in adults: preliminary report of an open-label and randomised phase 1 clinical trial
- PMID: 34324836
- PMCID: PMC8313090
- DOI: 10.1016/S1473-3099(21)00396-0
Safety, tolerability, and immunogenicity of an aerosolised adenovirus type-5 vector-based COVID-19 vaccine (Ad5-nCoV) in adults: preliminary report of an open-label and randomised phase 1 clinical trial
Abstract
Background: SARS-CoV-2 has caused millions of deaths, and, since Aug 11, 2020, 20 intramuscular COVID-19 vaccines have been approved for use. We aimed to evaluate the safety and immunogenicity of an aerosolised adenovirus type-5 vector-based COVID-19 vaccine (Ad5-nCoV) in adults without COVID-19 from China.
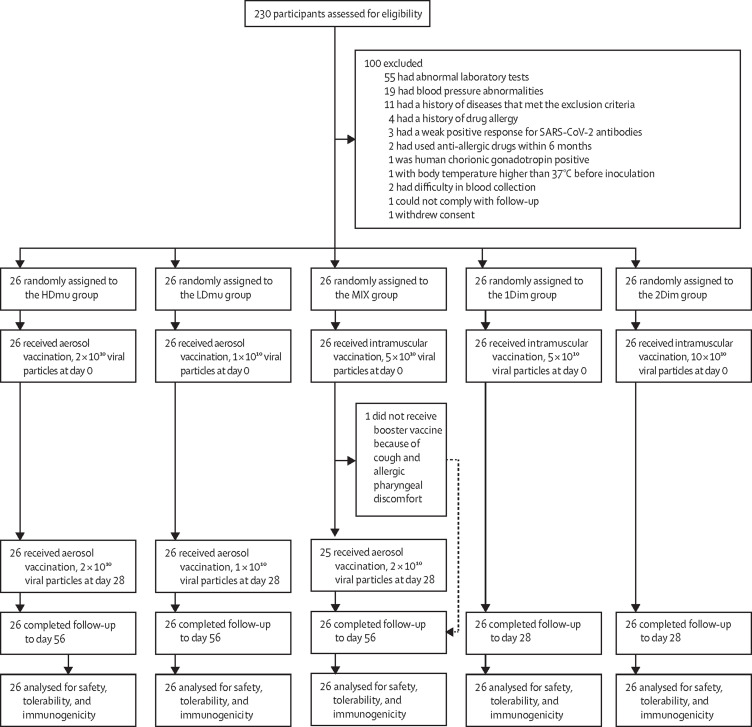
Method: This was a randomised, single-centre, open-label, phase 1 trial done in Zhongnan Hospital (Wuhan, China), to evaluate the safety and immunogenicity of the Ad5-nCoV vaccine by aerosol inhalation in adults (≥18 years) seronegative for SARS-CoV-2. Breastfeeding or pregnant women and people with major chronic illnesses or history of allergies were excluded. Participants were enrolled and randomly assigned (1:1:1:1:1) into five groups to be vaccinated via intramuscular injection, aerosol inhalation, or both. Randomisation was stratified by sex and age (18-55 years or ≥56 years) using computer-generated randomisation sequences (block sizes of five). Only laboratory staff were masked to group assignment. The participants in the two aerosol groups received an initial high dose (2 × 1010 viral particles; HDmu group) or low dose (1 × 1010 viral particles; LDmu group) of Ad5-nCoV vaccine on day 0, followed by a booster on day 28. The mixed vaccination group received an initial intramuscular (5 × 1010 viral particles) vaccine on day 0, followed by an aerosolised booster (2 × 1010 viral particles) vaccine on day 28 (MIX group). The intramuscular groups received one dose (5 × 1010 viral particles; 1Dim group) or two doses (10 × 1010 viral particles; 2Dim group) of Ad5-nCoV on day 0. The primary safety outcome was adverse events 7 days after each vaccination, and the primary immunogenicity outcome was anti-SARS-CoV-2 spike receptor IgG antibody and SARS-CoV-2 neutralising antibody geometric mean titres at day 28 after last vaccination. This trial is registered with ClinicalTrials.gov, number NCT04552366.
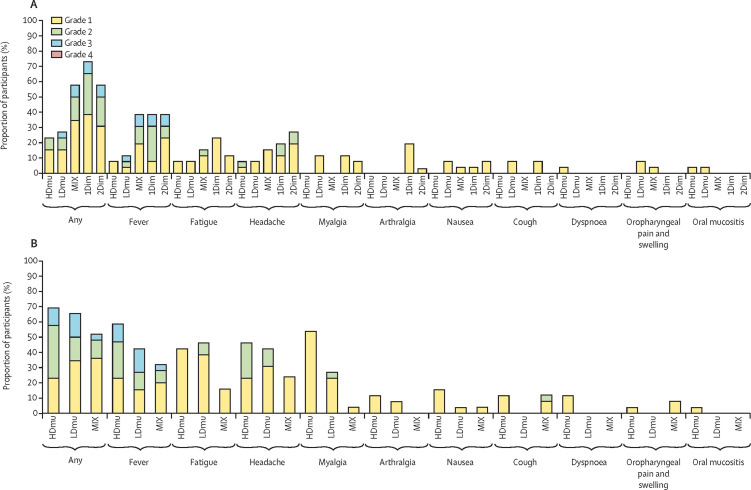
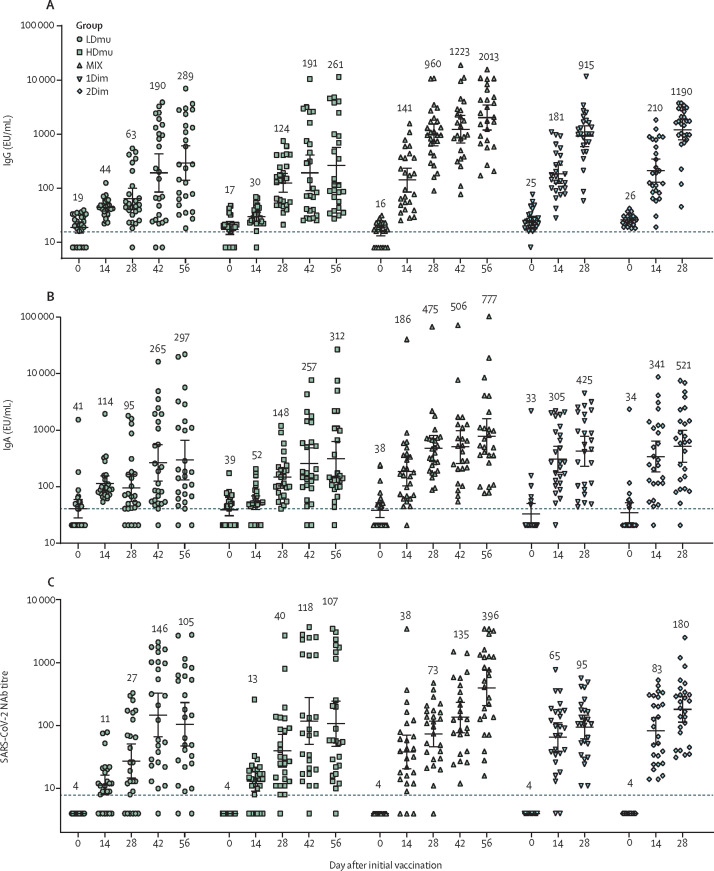
Findings: Between Sept 28, 2020, and Sept 30, 2020, 230 individuals were screened for inclusion, of whom 130 (56%) participants were enrolled into the trial and randomly assigned into one of the five groups (26 participants per group). Within 7 days after vaccination, adverse events occurred in 18 (69%) in the HDmu group, 19 (73%) in the LDmu group, 19 (73%) in the MIX group, 19 (73%) in the 1Dim group, and 15 (58%) in the 2Dim group. The most common adverse events reported 7 days after the first or booster vaccine were fever (62 [48%] of 130 participants), fatigue (40 [31%] participants), and headache (46 [35%] participants). More adverse events were reported in participants who received intramuscular vaccination, including participants in the MIX group (49 [63%] of 78 participants), than those who received aerosol vaccine (13 [25%] of 52 participants) after the first vaccine vaccination. No serious adverse events were noted within 56 days after the first vaccine. At days 28 after last vaccination, geometric mean titres of SARS-CoV-2 neutralising antibody was 107 (95% CI 47-245) in the HDmu group, 105 (47-232) in the LDmu group, 396 (207-758) in the MIX group, 95 (61-147) in the 1Dim group, and 180 (113-288) in the 2Dim group. The geometric mean concentrations of receptor binding domain-binding IgG was 261 EU/mL (95% CI 121-563) in the HDmu group, 289 EU/mL (138-606) in the LDmu group, 2013 EU/mL (1180-3435) in the MIX group, 915 EU/mL (588-1423) in the 1Dim group, and 1190 EU/mL (776-1824) in the 2Dim group.
Interpretation: Aerosolised Ad5-nCoV is well tolerated, and two doses of aerosolised Ad5-nCoV elicited neutralising antibody responses, similar to one dose of intramuscular injection. An aerosolised booster vaccination at 28 days after first intramuscular injection induced strong IgG and neutralising antibody responses. The efficacy and cost-effectiveness of aerosol vaccination should be evaluated in future studies.
Funding: National Key Research and Development Programme of China and National Science and Technology Major Project.
Translation: For the Chinese translation of the Summary see Supplementary Material.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests TZ, WS, JL are employees of CanSino Biologics. TZ has stock options in CanSino Biologics. All other authors declare no competing interests.
Figures
References
-
- COVID-19 Vaccine Tracker Vaccines candidates by trial phase. 2020. https://covid19.trackvaccines.org/vaccines
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
