

Prognostic Value of Minimal Left Atrial Volume in Heart Failure With Preserved Ejection Fraction
- PMID: 34325519
- PMCID: PMC8475710
- DOI: 10.1161/JAHA.120.019545
Prognostic Value of Minimal Left Atrial Volume in Heart Failure With Preserved Ejection Fraction
Abstract
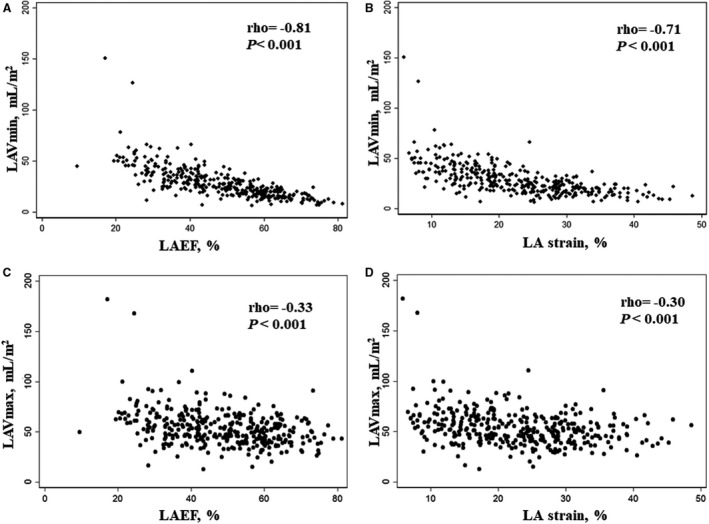
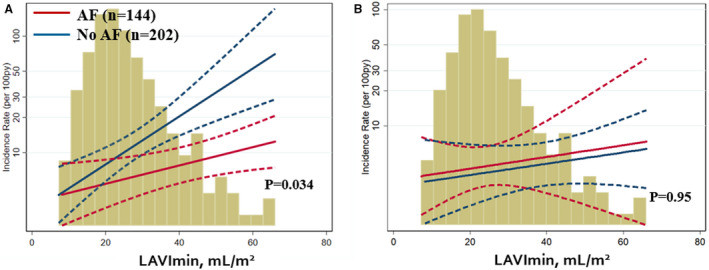
Background Maximal left atrial (LA) volume is reported by most echocardiography laboratories and is associated with clinical outcomes in patients with heart failure (HF). Recent studies suggest that minimal LA volume may better reflect left ventricular filling pressure and may be more prognostic than maximal LA volume. This study assessed the prognostic value of indexed minimal LA volume (LAVImin) in patients with HF with preserved ejection fraction. Methods and Results We assessed the relationship of LAVImin with a primary composite end point of cardiovascular death, aborted cardiac death, or HF hospitalization in 347 patients with HF with preserved ejection fraction enrolled from the Americas region in TOPCAT (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist Trial). We compared LAVImin with indexed maximal LA volume with respect to their prognostic values. In addition, we assessed if LA functional parameters provide additional prognostic information over LAVImin. During a median follow-up of 2.5 years, 107 patients (31%) experienced a primary composite end point. LAVImin was associated with increased risk of a primary composite outcome (hazard ratio [HR], 1.35; 95% CI, 1.12-1.61) and HF hospitalization alone (HR, 1.42; 95% CI, 1.17-1.71) after adjusting for clinical confounders and ejection fraction. In contrast, indexed maximal LA volume was not related to the primary composite outcome, but related to HF alone (HR, 1.25; 95% CI, 1.02-1.54). In comparison with indexed maximal LA volume, LAVImin was significantly more prognostic for primary composite outcome (P for comparison=0.032). Both LA emptying fraction and LA strain were prognostic of primary outcome independent of LAVImin (all P<0.05). Conclusions In patients with HF with preserved ejection fraction, LAVImin was more predictive of cardiovascular outcome than indexed maximal LA volume, suggesting this measure may be more physiologically relevant and might better identify patients at high risk for cardiovascular events. LA functional parameters provide prognostic information independent of LAVImin. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT00094302.
Keywords: cardiovascular outcomes; heart failure; left atrial volume; preserved ejection fraction.
Conflict of interest statement
Dr S.J. Shah has received research grants from the National Institutes of Health (NIH), Actelion, AstraZeneca, Corvia, and Novartis; and has served as a consultant or an Advisory Board member for Abbott, Actelion, AstraZeneca, Amgen, Bayer, Boehringer Ingelheim, Cardiora, Coridea, CVRx, Eisai, Ionis, Ironwood, Merck, MyoKardia, Novartis, Pfizer, Sanofi, Shifamed, Tenax, and United Therapeutics. Dr Zile has received grants and personal fees from Novartis, CVRx, and Medtronic; and has received personal fees from Abbott, Boston Scientific, EBR, Endotronics, Ironwood, Merck, Myokardia, and V Wave. Dr Pfeffer has received consulting fees from Amgen, AstraZeneca, Bayer, DalCor Pharma UK, Genzyme, Lilly, Medicines Company, MedImmune, Medtronic, Merck, Novartis, Novo Nordisk, Relypsa, Salix, Sanderling, Sanofi, Takeda, Teva, Thrasos, and Vericel; and has received research grant support from Amgen, Celladon, Novartis, and Sanofi. The Brigham and Women's Hospital has patents for the use of inhibitors of the renin‐angiotensin system in selected survivors of myocardial infarction with Novartis Pharmaceuticals, on which Dr Pfeffer is a coinventor. His share of the licensing agreement is irrevocably transferred to charity. Dr A.M. Shah has received grants from NIH/National Heart, Lung, and Blood Institute (NHLBI); has received research support from Novartis through Brigham and Women's Hospital; and has received consulting fees from Philips Ultrasound and Bellerophon Therapeutics. Dr Solomon has received research grants from Alnylam, Amgen, AstraZeneca, Bellerophon, Celladon, Gilead, GSK, Ionis Pharmaceutics, Lone Star Heart, Mesoblast, MyoKardia, NIH/NHLBI, Novartis, Sanofi Pasteur, and Theracos; and has consulted for Alnylam, Amgen, AstraZeneca, Bayer, BMS, Corvia, Gilead, GSK, Ironwood, Merck, Novartis, Pfizer, Takeda, and Theracos. The remaining authors have no disclosures to report.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola V‐P, Jankowska EA, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. DOI: 10.1093/eurheartj/ehw128. - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, et al. Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation. 2011;124:2491–2501. DOI: 10.1161/CIRCULATIONAHA.110.011031. - DOI - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, et al. Atrial fibrillation and risk of clinical events in chronic heart failure with and without left ventricular systolic dysfunction: results from the Candesartan in Heart failure‐Assessment of Reduction in Mortality and morbidity (CHARM) program. J Am Coll Cardiol. 2006;47:1997–2004. DOI: 10.1016/j.jacc.2006.01.060. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
