

Durable responses in patients with genitourinary cancers following immune checkpoint therapy rechallenge after moderate-to-severe immune-related adverse events
- PMID: 34326169
- PMCID: PMC8323401
- DOI: 10.1136/jitc-2021-002850
Durable responses in patients with genitourinary cancers following immune checkpoint therapy rechallenge after moderate-to-severe immune-related adverse events
Abstract
Background: Immune checkpoint therapy (ICT) prolongs survival in subsets of patients with cancer but can also trigger immune-related adverse events (irAEs) requiring treatment discontinuation. Recent studies have investigated safety of ICT rechallenge after irAEs, and evidence suggests that rechallenge may be associated with improved antitumor responses. However, data are limited on response duration after ICT rechallenge, particularly after severe irAEs.
Objective: To evaluate safety and efficacy of ICT rechallenge after moderate-to-severe irAEs in patients with renal cell carcinoma (RCC), urothelial carcinoma (UC), and prostate cancer.
Methods: In this retrospective cohort study, medical records from September 25, 2013, to June 1, 2020, for patients with genitourinary (GU) cancers at MD Anderson Cancer Center who were rechallenged with the same or different ICT following irAEs were reviewed. Demographics, ICT exposure, irAEs (grade and treatment), ICT discontinuation or rechallenge, rates of subsequent irAEs (new or recurrent) and antitumor activity (objective response rates and response duration) were reviewed.
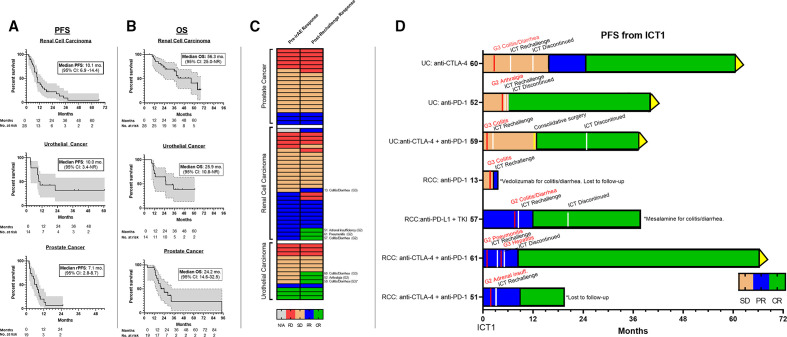
Results: Sixty-one patients with RCC, UC, and prostate cancer were rechallenged with ICT after experiencing 105 total irAEs. Objective response rates after rechallenge, that is, upgrade in response, were 14% in RCC (4/28), 21% in UC (3/14), and 0% in prostate cancer. All seven patients who achieved upgrade in response had initial grade 2 or 3 irAEs. Responses were durable among these seven patients, with median radiographic progression-free survival not reached (range: 3.7-66.4 months) as of the March 8, 2021, data cut-off (median follow-up 40.9 months (95% CI 35.3 to 46.5)). All achieved complete response except one patient who was lost to follow-up. The rate of subsequent grade 3 or 4 irAEs after rechallenge was 30%, with no fatal irAEs. The rate of recrudescence of the same irAE was 26% (16/61). 54% of patients received corticosteroids (33/61), and 21% received targeted immunosuppression (13/61) for the initial irAEs.
Conclusions and relevance: ICT rechallenge after moderate-to-severe irAEs was associated with deep and durable responses in a subset of patients with RCC and UC, with acceptable safety and no fatal events. Strategies to enable ICT resumption after moderate-to-severe irAEs, such targeted immunosuppression, warrant further study.
Keywords: autoimmunity; immunotherapy; kidney neoplasms; prostatic neoplasms; urinary bladder neoplasms.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: BAS, JSG, RG, TKB, DSS, JW, SG, and PGC report no relevant disclosures. AYS reports advisory board disclosures for Exelixis, Bristol Myers Squibb, Roche, and Pfizer; and research disclosures from Eisai, Bristol Myers Squibb, and EMD Serono. MTC reports Advisory Board/Honararium: Eisai, Exelixis, Seattle Genetics, Astellas, Pfizer, EMD Serono; Research Funding: Janssen, Exelixis, EMD Serono, Pfizer, Apricity Health, AstraZeneca. PM has received honoraria for service on a scientific advisory boards for Mirati Therapeutics, Bristol-Myers Squibb, and Exelixis; consulting for Axiom Healthcare Strategies; non-branded educational programs supported by Exelixis and Pfizer; and research funding for clinical trials from Takeda, Bristol-Myers Squibb, Mirati Therapeutics, Gateway for Cancer Research, and UT MD Anderson Cancer Center. EJ reports research funding: Aravive, Arrowhead, Merck, Novartis; honoraria: Aravive, Eisai, Exelixis, Ipsen, Merck, NiKang, Novartis, Pfizer. AJZ reports consulting or advisory roles for AstraZeneca and Bayer; research funding to his institution from Infinity Pharma; honoraria from Pfizer and Janssen. AMA reports Consulting/Advisory Board: Daiichi Sankyo, AstraZeneca, Amgen, Janssen, Astellas, Genzyme; Editorial Role: American Cancer Society. AOS-R reports: Consulting/Advisory/Speaker: AstraZeneca, Basilea, Bristol Myers Squibb, Merck, Mirati, Nektar, Seattle Genetics, Taiho, Janssen, Immunomedics; Research Funding: Basilea, Bristol Myers Squibb, Merck, Netkar, Janssen, Immunomedics. PS reports Stock/Other Ownership: Achelois, Adaptive Biotechnologies, Affini-T, Apricity Health, BioAtla, BioNTech, Codiak Biosciences, Constellation, Dragonfly Therapeutics, Earli, Glympse, Hummingbird Biosciences, ImaginAB, Infinity Pharma, Jounce Therapeutics, JSL Health, Lava Therapeutics, Lytix Biopharma, Marker Therapeutics, Oncolytics, PBM Capital, Phenomics, Polaris Group, Sporos, Time Bioventures; Consulting/Advisory Role: Achelois, Affini-T, Apricity Health, BioAtla, Codiak Biosciences, Dragonfly Therapeutics, Earli, Glympse, Hummingbird Biosciences, ImaginAB, Infinity Pharma, Jounce Therapeutics, JSL Health, Lava Therapeutics, Lytix Biopharma, Marker Therapeutics, Oncolytics, PBM Capital, Phenomics, Polaris Group, Sporos, Time Bioventures. SKS reports Stock and Other Ownership Interests: Apricity Health; Honoraria: Apricity Health, Janssen, Dendreon, Polaris, Parker Institute of Cancer Immunotherapy, Amgen, AstraZeneca, Bayer, Bristol Myers Squibb, Dava Oncology, Exelixis, Society for Immunotherapy of Cancer; Consulting or Advisory Role: Valeant/Dendreon, Apricity Health, Janssen, Polaris, Bayer, Bristol Myers Squibb, Amgen, AstraZeneca, Dava Oncology; Research Funding: Janssen, Bristol Myers Squibb, AstraZeneca; Travel, Accommodations, Expenses: Janssen, Compugen, Dendreon, Amgen, Parker Institute for Cancer Immunotherapy, Bristol Myers Squibb, Society for Immunotherapy of Cancer, AstraZeneca, Dava Oncology. NMT reports consulting/advisory relationship: Bristol Myers Squibb; Pfizer; Nektar Therapeutics; Exelisis, Eisai Medical Research; Eli Lilly; Oncorena; Calithera Bioscience; Surface Oncology; Novartis, Ipsen; Merck Sharp & Dohme; Research Funding: Bristol Myers Squibb; Nektar Therapeutics; Calithera Bioscience; Arrowhead Pharmaceuticals; Scientific Advisory Committees: Nektar Therapeutics; Pfizer, Oncorena; Eli Lilly, Eisai Medical Research.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical