

SARS-CoV-2 specific T cell responses are lower in children and increase with age and time after infection
- PMID: 34326343
- PMCID: PMC8322064
- DOI: 10.1038/s41467-021-24938-4
SARS-CoV-2 specific T cell responses are lower in children and increase with age and time after infection
Abstract
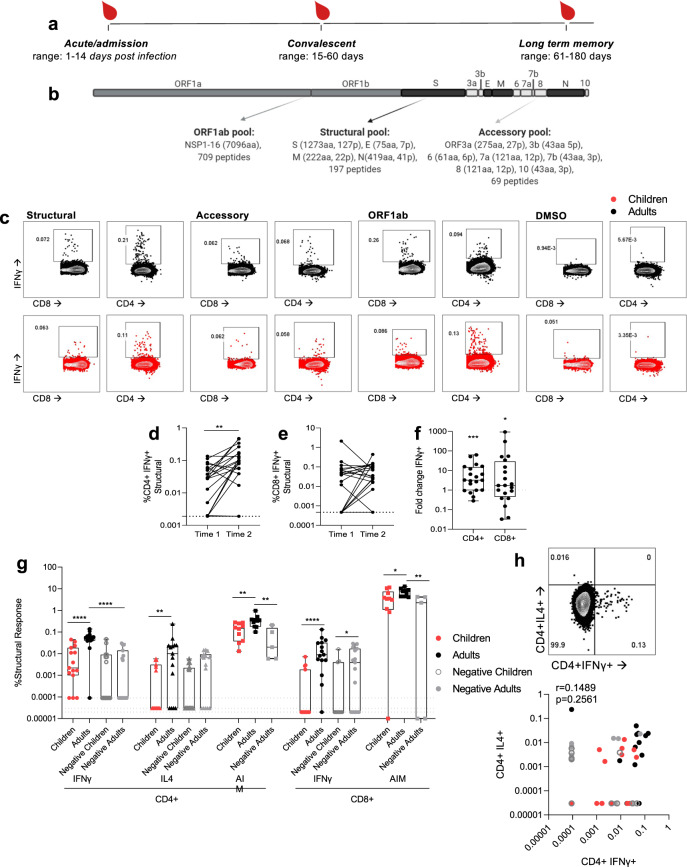
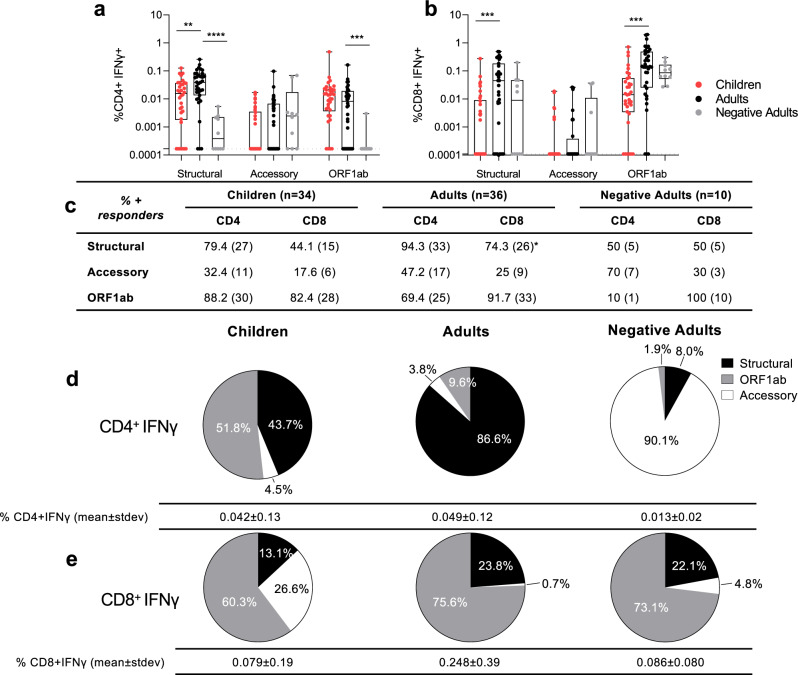
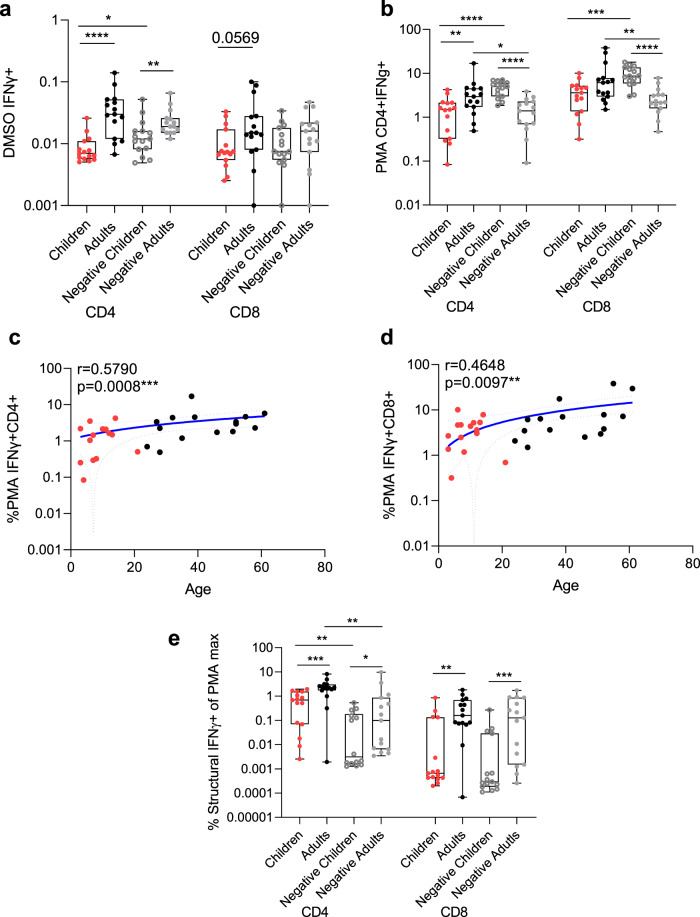
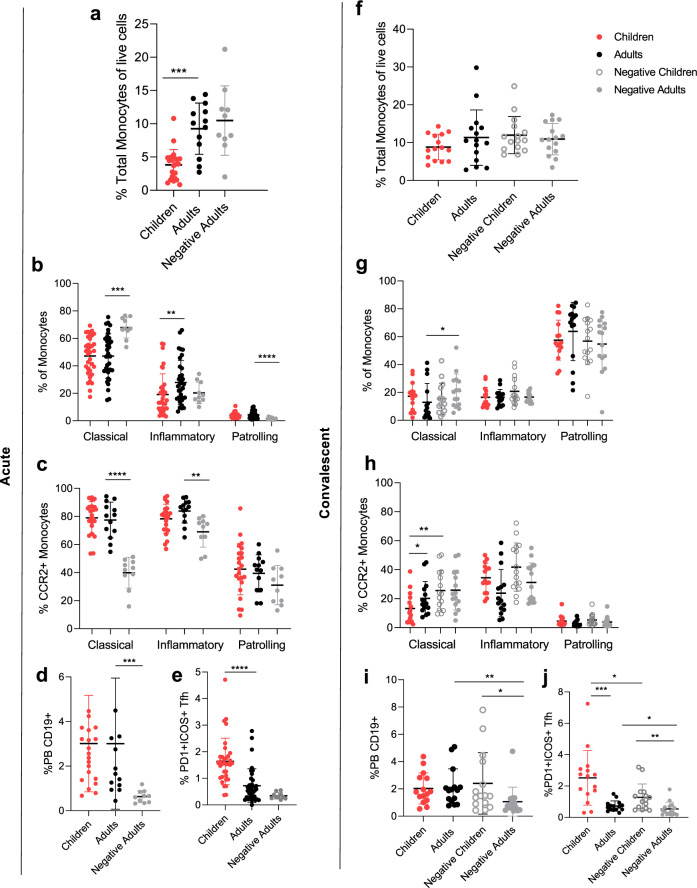
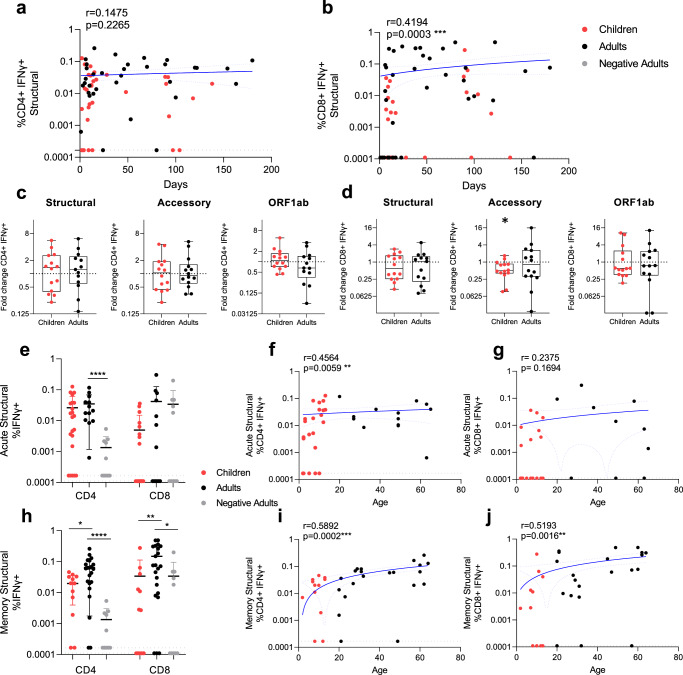
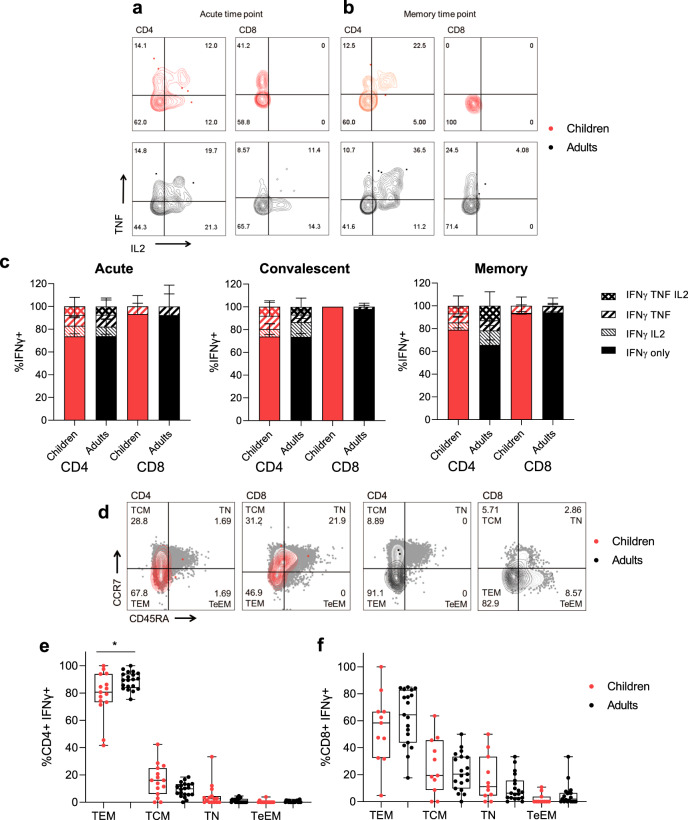
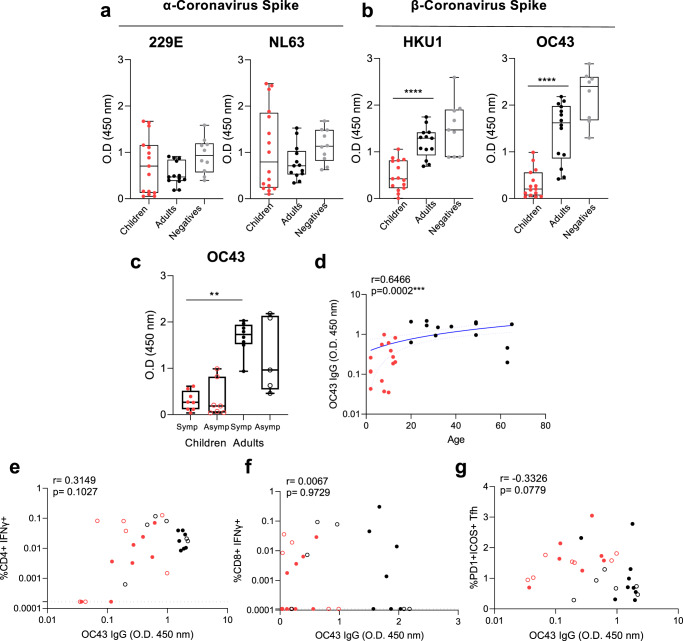
SARS-CoV-2 infection of children leads to a mild illness and the immunological differences with adults are unclear. Here, we report SARS-CoV-2 specific T cell responses in infected adults and children and find that the acute and memory CD4+ T cell responses to structural SARS-CoV-2 proteins increase with age, whereas CD8+ T cell responses increase with time post-infection. Infected children have lower CD4+ and CD8+ T cell responses to SARS-CoV-2 structural and ORF1ab proteins when compared with infected adults, comparable T cell polyfunctionality and reduced CD4+ T cell effector memory. Compared with adults, children have lower levels of antibodies to β-coronaviruses, indicating differing baseline immunity. Total T follicular helper responses are increased, whilst monocyte numbers are reduced, indicating rapid adaptive co-ordination of the T and B cell responses and differing levels of inflammation. Therefore, reduced prior β-coronavirus immunity and reduced T cell activation in children might drive milder COVID-19 pathogenesis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Update of
-
SARS-CoV-2 specific T cell responses are lower in children and increase with age and time after infection.medRxiv [Preprint]. 2021 Feb 5:2021.02.02.21250988. doi: 10.1101/2021.02.02.21250988. medRxiv. 2021. Update in: Nat Commun. 2021 Jul 29;12(1):4678. doi: 10.1038/s41467-021-24938-4. PMID: 33564773 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
