

Dialysis adequacy predictions using a machine learning method
- PMID: 34326393
- PMCID: PMC8322325
- DOI: 10.1038/s41598-021-94964-1
Dialysis adequacy predictions using a machine learning method
Abstract
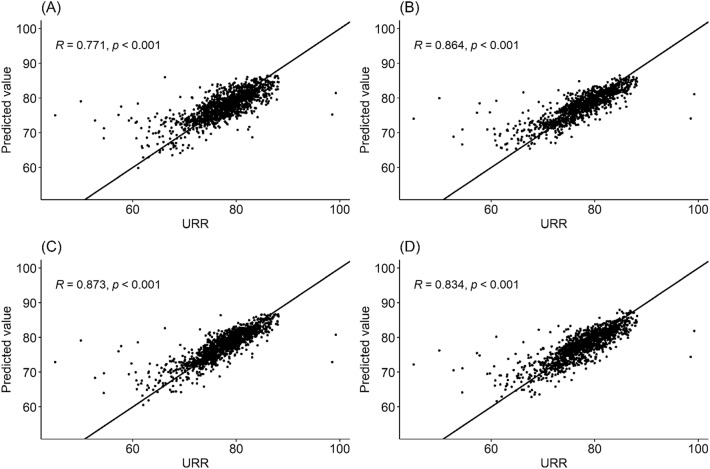
Dialysis adequacy is an important survival indicator in patients with chronic hemodialysis. However, there are inconveniences and disadvantages to measuring dialysis adequacy by blood samples. This study used machine learning models to predict dialysis adequacy in chronic hemodialysis patients using repeatedly measured data during hemodialysis. This study included 1333 hemodialysis sessions corresponding to the monthly examination dates of 61 patients. Patient demographics and clinical parameters were continuously measured from the hemodialysis machine; 240 measurements were collected from each hemodialysis session. Machine learning models (random forest and extreme gradient boosting [XGBoost]) and deep learning models (convolutional neural network and gated recurrent unit) were compared with multivariable linear regression models. The mean absolute percentage error (MAPE), root mean square error (RMSE), and Spearman's rank correlation coefficient (Corr) for each model using fivefold cross-validation were calculated as performance measurements. The XGBoost model had the best performance among all methods (MAPE = 2.500; RMSE = 2.906; Corr = 0.873). The deep learning models with convolutional neural network (MAPE = 2.835; RMSE = 3.125; Corr = 0.833) and gated recurrent unit (MAPE = 2.974; RMSE = 3.230; Corr = 0.824) had similar performances. The linear regression models had the lowest performance (MAPE = 3.284; RMSE = 3.586; Corr = 0.770) compared with other models. Machine learning methods can accurately infer hemodialysis adequacy using continuously measured data from hemodialysis machines.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
