

Long-Term Mechanical Ventilation in Neonates: A 10-Year Overview and Predictive Model
- PMID: 34327181
- PMCID: PMC8313736
- DOI: 10.3389/fped.2021.689190
Long-Term Mechanical Ventilation in Neonates: A 10-Year Overview and Predictive Model
Abstract
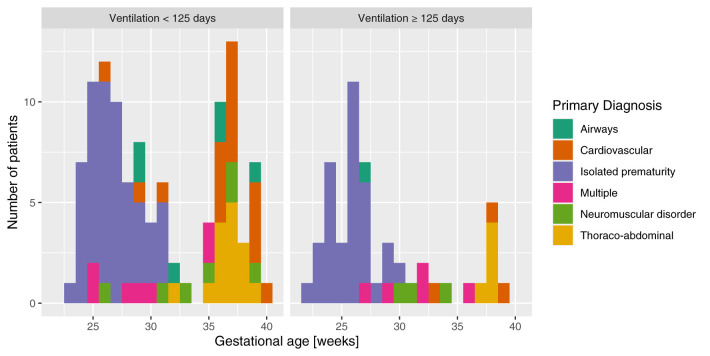
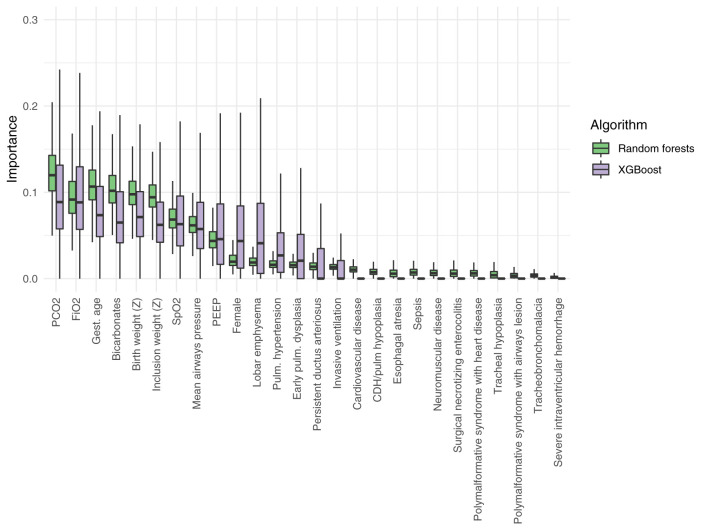
Objectives: Significant resources are devoted to neonatal prolonged mechanical ventilation (NPMV), but little is known about the outcomes in those children. Our primary objective was to describe the NPMV respiratory, digestive, and neurological outcomes at 18 months corrected age. Our second objective was on the early identification of which patients, among the NPMV cohort, will need to be ventilated for ≥125 days, which corresponded to the 75th percentile in the preliminary data, and to describe that subgroup. Methods: In this retrospective cohort study, we included all children born between 2004 and 2013 who had a NPMV (≥21 days of invasive or noninvasive respiratory support reached between 40 and 44 weeks of postconceptional age). We used random forests, logistic regression with penalization, naive Bayes, and XGBoost to predict which patients will need ≥125 days of ventilation. We used a Monte Carlo cross validation. Results: We included 164 patients. Of which, 40% (n = 66) were female, and the median gestational age was 29 weeks [interquartile range (IQR): 26-36 weeks] with a bimodal distribution. Median ventilation days were 104 (IQR: 66-139 days). The most frequently associated diagnoses were pulmonary hypertension (43%), early pulmonary dysplasia (41%), and lobar emphysema (37%). At 18 months corrected age, 29% (n = 47) had died, 59% (n = 97) were free of any respiratory support, and 45% (n = 74) were exclusively orally fed. A moderate area under the ROC curve of 0.65 (95% CI: 0.54-0.72) for identifying patients in need of ≥125 days of ventilation at inclusion was achieved by random forests classifiers. Among the 26 measured at inclusion, the most contributive ones were PCO2, inspired O2 concentration, and gestational age. At 18 months corrected age, patients ventilated for ≥125 days had a lower respiratory weaning success (76 vs. 87%, P = 0.05), lower exclusive oral feeding proportion (51 vs. 84%, P < 0.001), and a higher neurological impairment (median Pediatric Cerebral Performance Category score 3 vs. 2, P = 0.008) than patients ventilated for < 125 days. Conclusion: NPMV is a severe condition with a high risk of mortality, neurological impairment, and oral feed delay at 18 months. Most survivors are weaned of any respiratory support. We identified the risk factors that allow for the early identification of the most at-risk children of long-term ventilation with a moderate discrimination.
Keywords: children; clinical decision support; critical care; hospital mortality; machine learning; prolonged mechanical ventilation.
Copyright © 2021 Sauthier, Sauthier, Bergeron Gallant, Lodygensky, Kawaguchi, Emeriaud and Jouvet.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor declared a past co-authorship with one of the authors GE.
Figures
References
LinkOut - more resources
Full Text Sources