

Diabetes during pregnancy and birthweight trends among Aboriginal and non-Aboriginal people in the Northern Territory of Australia over 30 years
- PMID: 34327339
- PMCID: PMC8315488
- DOI: 10.1016/j.lanwpc.2020.100005
Diabetes during pregnancy and birthweight trends among Aboriginal and non-Aboriginal people in the Northern Territory of Australia over 30 years
Abstract
Background: Early-life risk factors, including maternal hyperglycaemia and birthweight, are thought to contribute to the high burden of cardiometabolic disease experienced by Indigenous populations. We examined rates of pre-existing diabetes in pregnancy, gestational diabetes mellitus (GDM) and extremes of birthweight over three decades in the Northern Territory (NT) of Australia.
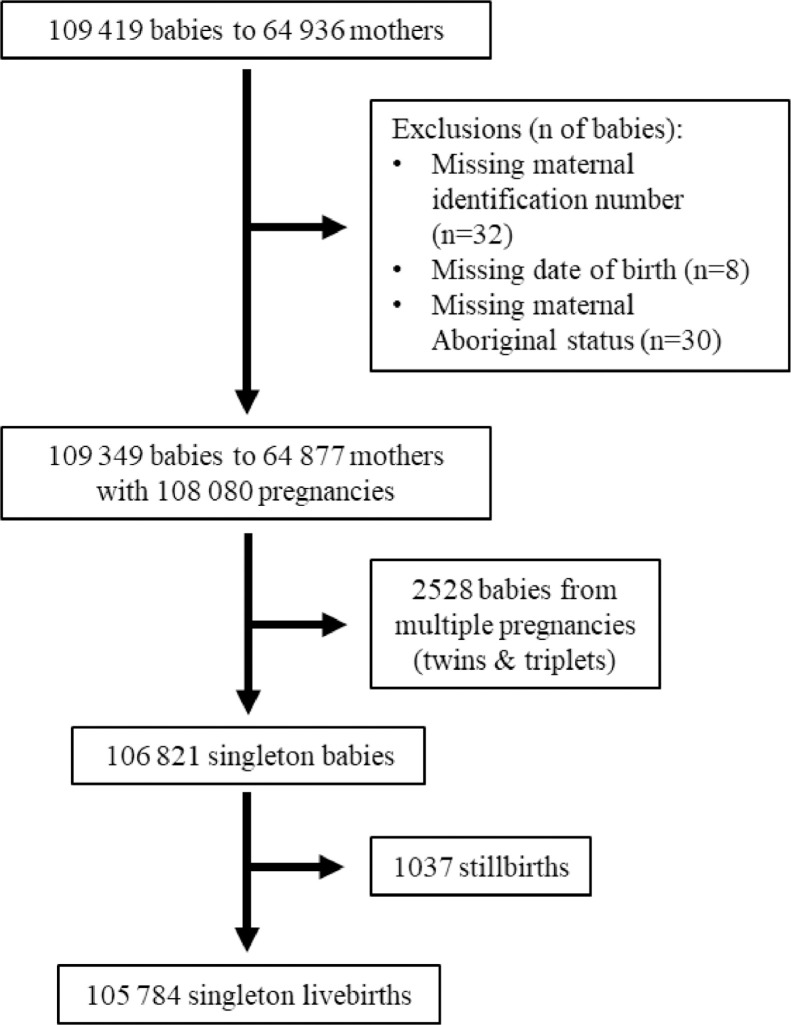
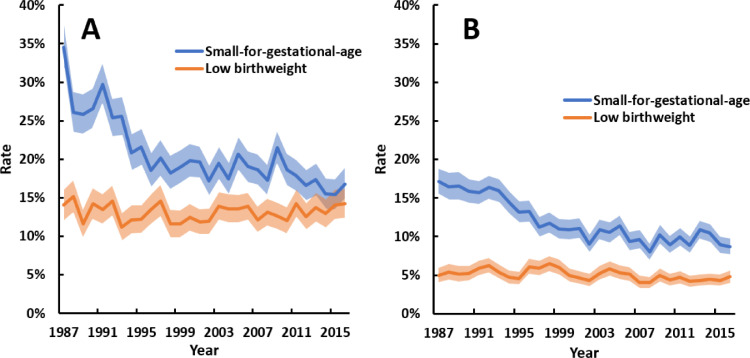
Methods: We performed a retrospective cohort analysis of the NT Perinatal Data Collection from 1987 to 2016, including all births >20 weeks gestation, stratified by maternal Aboriginal identification. Key outcomes were annual rates of pre-existing diabetes, GDM, small-for-gestational-age, large-for-gestational-age, low birthweight (<2500 g), and high birthweight (>4000 g). Logistic regression was used to assess trends and interactions.
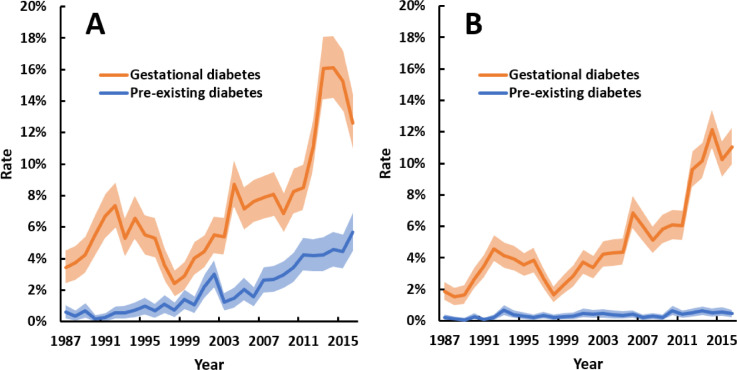
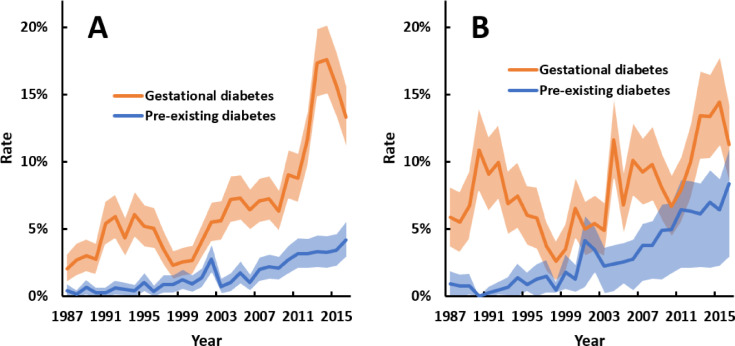
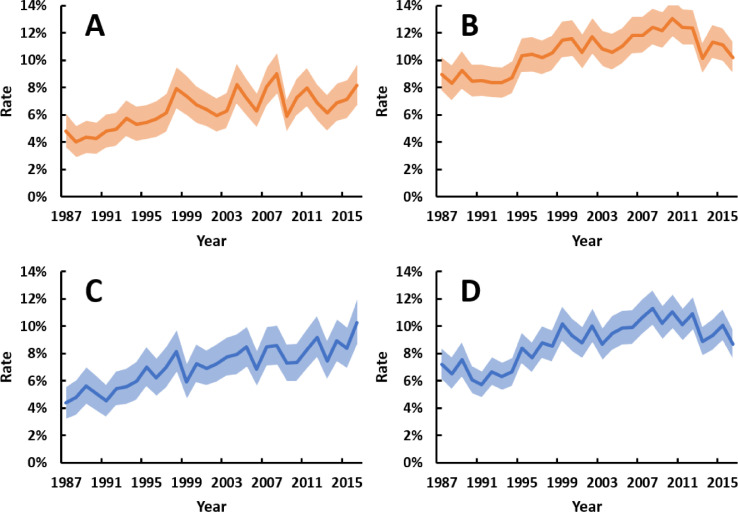
Findings: 109 349 babies were born to 64 877 mothers, 36% of whom identified as Aboriginal ethnicity. Among Aboriginal women, rates of GDM and pre-existing diabetes, respectively, were 3 · 4% and 0 · 6% in 1987 and rose to 13% and 5 · 7% in 2016 (both trends p<0 · 001). Among non-Aboriginal women, rates of GDM increased from 1 · 9% in 1987 to 11% in 2016 (p<0 · 001), while pre-existing diabetes was uncommon (≤0 · 7% throughout). Rates of small-for-gestational-age decreased, while rates of large-for-gestational-age and high birthweight increased in both groups (all trends p<0 · 001). Multivariable modelling suggests that hyperglycaemia was largely responsible for the growing rate of large-for-gestational-age births among Aboriginal women.
Interpretation: The burden of hyperglycaemia in pregnancy has grown substantially in the NT over three decades and is impacting birthweight trends. The prevalence of pre-gestational diabetes in Aboriginal women is among the highest in the world.
Funding: Diabetes Australia Research Program.
© 2020 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
MJLH, FB, SG, RFD, ELMB, GS, VW, JES and LJMB report a competitive grant from the Diabetes Australia Research Program for this study. MJLH also reports scholarship support from the National Health and Medical Research Council (NHMRC), Diabetes Australia and the Australian Academy of Science. JAB, JES and LJMB also report competitive fellowships or grants from the NHMRC. JES has received honoraria for lectures and consultancies unrelated to this study from AstraZeneca, Eli Lilly, Mylan, Novo Nordisk, Sanofi, Merck Sharp and Dohme, Abbott and Boehringer Ingelheim.
Figures
References
-
- Naqshbandi M., Harris S.B., Esler J.G., Antwi-Nsiah F. Global complication rates of type 2 diabetes in Indigenous peoples: a comprehensive review. Diabetes Res Clin Pract. 2008;82(1):1–17. - PubMed
-
- McNamara B.J., Gubhaju L., Chamberlain C., Stanley F., Eades S.J. Early life influences on cardio-metabolic disease risk in aboriginal populations – what is the evidence? A systematic review of longitudinal and case-control studies. Int J Epidemiol. 2012;41(6):1661–1682. - PubMed
-
- Maple-Brown L., Lee I.L., Longmore D. Pregnancy and neonatal diabetes outcomes in remote Australia: the PANDORA study-an observational birth cohort. Int J Epidemiol. 2019;48(1):307–318. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
