

Hepatitis C elimination in Myanmar: Modelling the impact, cost, cost-effectiveness and economic benefits
- PMID: 34327345
- PMCID: PMC8315611
- DOI: 10.1016/j.lanwpc.2021.100129
Hepatitis C elimination in Myanmar: Modelling the impact, cost, cost-effectiveness and economic benefits
Abstract
Background: Myanmar has set national hepatitis C (HCV) targets to achieve 50% of people diagnosed and 50% treated by 2030. The WHO has additional targets of reducing incidence by 80% and mortality by 65% by 2030. We aimed to estimate the impact, cost, cost-effectiveness and net economic benefit of achieving these targets.
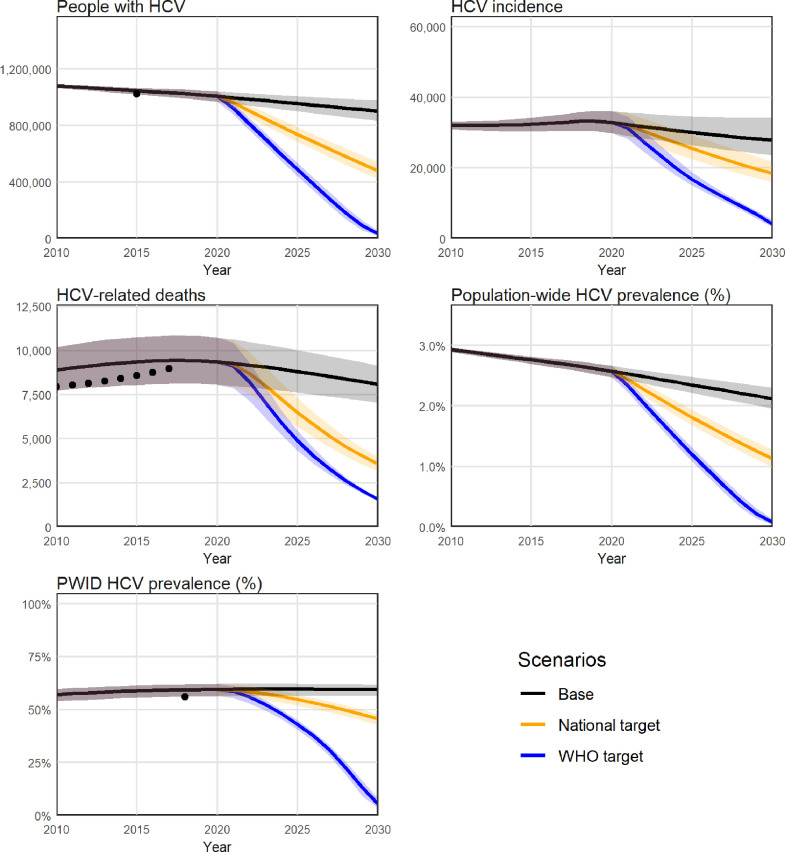
Methods: Mathematical models of HCV transmission, disease progression and the care cascade were calibrated to 15 administrative regions of Myanmar. Cost data were collected from a community testing and treatment program in Yangon. Three scenarios were projected for 2020-2030: (1) baseline (current levels of testing/treatment); and testing/treatment scaled up sufficiently to reach (2) the national strategy targets; and (3) the WHO targets.
Findings: Without treatment scale-up, 333,000 new HCV infections and 97,000 HCV-related deaths were estimated to occur in Myanmar 2020-2030, with HCV costing a total $100 million in direct costs (testing, treatment, disease management) and $10.4 billion in lost productivity. In the model, treating 55,000 people each year was sufficient to reach the national strategy targets and prevented a cumulative 40,000 new infections (12%) and 25,000 HCV-related deaths (25%) 2020-2030. This was estimated to cost a total $189 million in direct costs ($243 per DALY averted compared to no treatment scale-up), but only $9.8 billion in lost productivity, making it cost-saving from a societal perspective by 2024 with an estimated net economic benefit of $553 million by 2030. Reaching the WHO targets required further treatment scale-up and additional direct costs but resulted in greater longer-term benefits.
Interpretation: Current levels of HCV testing and treatment in Myanmar are insufficient to reach the national strategy targets. Scaling up HCV testing and treatment in Myanmar to reach the national strategy targets is estimated to generate significant health and economic benefits.
Funding: Gilead Sciences.
Keywords: Elimination; Hepatitis C; Low and middle income country; Mathematical model; Myanmar.
© 2021 The Author(s).
Conflict of interest statement
NS and the Burnet Institute received investigator-initiated research funding from Gilead Sciences for this work. KPK receives non-financial support from Mylan Myanmar, Hetero Pharmaceutical, and Royal Ruby Co. Ltd. WN received non-financial support from Mylan Myanmar and Cipla Pharmaceutical. MH receives investigator-initiated research funding from Gilead Sciences and AbbVie outside of this work. TMW, TT, HH, BD, PTZA, YX, AB, CK, SS, KSA have nothing to declare.
Figures




References
-
- World Health Organization. Hepatitis C fact sheet. 2017.
-
- World Health Organization . 2017. Global Hepatitis Report 2017. Geneva. Licence: CC BY-NC-SA 3.0 IGO.
-
- Lawitz E., Poordad F.F., Pang P.S. Sofosbuvir and ledipasvir fixed-dose combination with and without ribavirin in treatment-naive and previously treated patients with genotype 1 hepatitis C virus infection (LONESTAR): an open-label, randomised, phase 2 trial. Lancet. 2014;383(9916):515–523. - PubMed
LinkOut - more resources
Full Text Sources
