

Risk of female-specific cancers according to obesity and menopausal status in 2•7 million Korean women: Similar trends between Korean and Western women
- PMID: 34327357
- PMCID: PMC8315398
- DOI: 10.1016/j.lanwpc.2021.100146
Risk of female-specific cancers according to obesity and menopausal status in 2•7 million Korean women: Similar trends between Korean and Western women
Abstract
Background: Studies examining the relationship between obesity and female-specific cancers have been mainly conducted in Western populations. We aimed to investigate the risk of female-specific cancers according to obesity and menopausal status using a nationwide cohort in Korea.
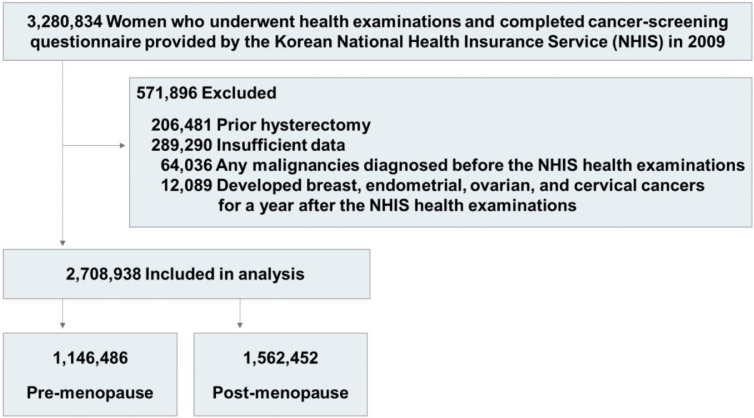
Methods: We identified 2,708,938 women from the National Health Insurance Service cohort, and obtained baseline body mass index (BMI), waist circumference (WC), and other healthcare data, measured and collected during a health examinations and cancer-screening survey. By setting a normal weight/WC group (BMI, 18•5-22•9 kg/m2 or WC, 80•0-84•9 cm) as the reference, we conducted multivariate analyses using the Cox proportional hazard model to estimate adjusted hazard ratios (aHRs) and 95% confidence intervals (95% CIs) for each cancer.
Findings: The total follow-up duration was 22389854•63 person-years. In post-menopausal women, the risk of breast, endometrial, and ovarian cancers significantly increased as the BMI classification level increased from normal to class II obesity (aHRs [95% CIs], 1•49 [1•38-1.61], 2•11 [1•81-2•46], and 1•38 [1•20-1•58], respectively). The risk of breast and endometrial cancers also increased as the WC classification increased from < 75•0 to ≥ 95•0 cm. With a WC of 80•0-84•9 cm as the reference, the lowest risk of breast and endometrial cancers was observed in WC < 75•0 cm (aHRs [95% CIs], 0•85 [0•81-0•89] and 0•75 [0•67-0•84], respectively) while the highest risk was observed in WC ≥ 95•0 cm (aHRs [95% CIs], 1•19 [1•10-1•29] and 1•56 [1•33-1•82], respectively). In pre-menopausal women, the risk of breast cancer significantly decreased in those with class I and II obesity compared to those with normal BMI (aHRs [95% CIs], 0•96 [0•92-0•999] and 0•89 [0•81-0•97], respectively), whereas the trends of endometrial and ovarian cancer incidence in pre-menopausal women were similar to those observed in post-menopausal women. For cervical cancer, only class II obesity was significantly associated with increased risks in both post-menopausal and pre-menopausal women (aHRs [95% CIs], 1•18 [1•01-1•39] and 1•27 [1•02-1•57], respectively).
Interpretation: In this large population-based cohort study in Korean women, we observed that the impact of obesity on the development of female-specific cancers differs according to the malignancy type and menopausal status. Similar trends were observed between Korean and Western women.
Funding: The Korea Health Industry Development Institute (no. HI16C2037).
Keywords: Body mass index; Breast cancer; Cervical cancer; Endometrial cancer; Incidence; Menopause; Obesity; Ovarian cancer; Waist circumference.
© 2021 Published by Elsevier Ltd.
Conflict of interest statement
All authors declare no competing interests.
Figures




References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–591. - PubMed
-
- Enriori CL, Reforzo-Membrives J. Peripheral aromatization as a risk factor for breast and endometrial cancer in postmenopausal women: a review. Gynecol Oncol. 1984;17(1):1–21. - PubMed
LinkOut - more resources
Full Text Sources
