

Anthracycline-free or short-term regimen as adjuvant chemotherapy for operable breast cancer: A phase III randomized non-inferiority trial
- PMID: 34327363
- PMCID: PMC8315472
- DOI: 10.1016/j.lanwpc.2021.100158
Anthracycline-free or short-term regimen as adjuvant chemotherapy for operable breast cancer: A phase III randomized non-inferiority trial
Abstract
Background: De-escalating anthracycline is gaining popularity for breast cancer patients. We aim to evaluate the non-inferiority of an anthracycline-free or short-term regimen to the standard anthracycline-based regimen for operable patients with human epidermal growth factor receptor 2 (HER2)-negative breast cancer.
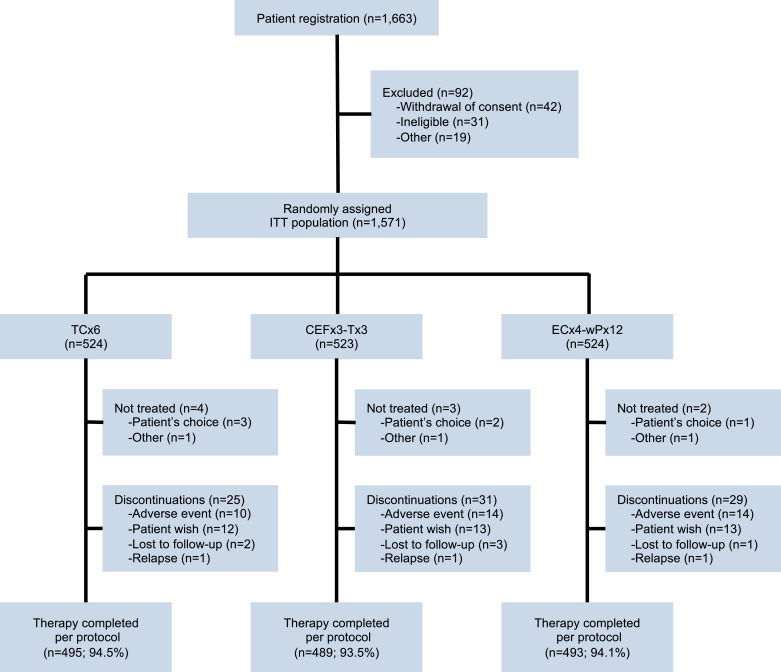
Methods: It is a prospective, open-label, phase 3, randomized non-inferiority trial from June 1, 2010 to June 1, 2017. Follow-up had been kept until July 2019. This trial was conducted at Fudan University Shanghai Cancer Center. Patients with pT1-3N+ or pT2-3N0 but high-risk (grade II/III, lymphovascular invasion, ≤35 years of age or hormone-receptor negative) HER2-negative operable breast cancer were eligible and stratified by age, pathological tumour stage, pathological node status and hormone-receptor status. Patients were randomized to 6 cycles of docetaxel and cyclophosphamide (TC, n = 524), 3 cycles of cyclophosphamide/epirubicin/fluorouracil followed by 3 cycles of docetaxel (CEF-T, n = 523) or epirubicin and cyclophosphamide for 4 cycles followed by paclitaxel for 12 weeks (EC-P, n = 524) as the intention-to-treat population. Of these patients, 94% completed allocated therapy. Difference in disease-free survival (DFS) compared to EC-P. The prespecified non-inferiority margin was 4.5%, corresponding to the hazard ratio (HR) of 1.44 (one-sided α = 0.05), with an assumed 5-year DFS of 89% for EC-P.
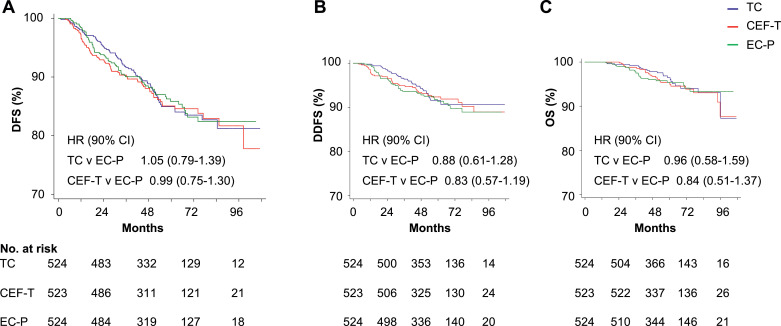
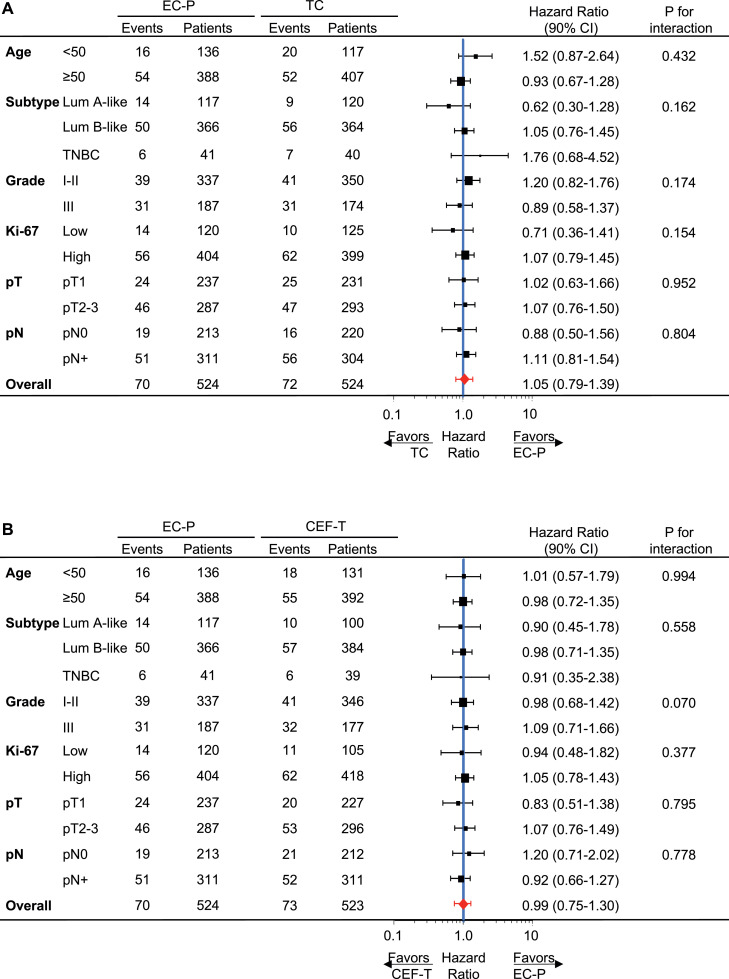
Findings: Included in the intention-to-treat population were 1571 patients (median [IQR] age, 50 [45-57] years; 92% estrogen receptor [ER]-positive; 59% pN+). Through a median follow-up of 5.5 years, HR for TC versus EC-P was 1.05 (5-year DFS: 85.0% vs. 85.9%; 90% confidence interval [CI]: 0.79-1.39, non-inferior P = 0.048) and for CEF-T versus EC-P, 0.99 (5-year DFS: 85.1% vs. 85.9%; 90% CI: 0.75-1.30, non-inferior P = 0.045). Grade 3 or 4 adverse events for TC included rash (3.9%) and peripheral neuropathy (2.8%) and for CEF-T and EC-P diarrhea and nausea/vomiting were predominant. Results of per-protocol analyses were similar.
Interpretation: Both TC and CEF-T are non-inferior adjuvant regimen to EC-P mainly in patients with ER+HER2- breast cancer. TC is a safe regimen that avoids anthracycline-related side effects.
Funding: This work was supported by grants from the National Natural Science Foundation of China (Grants 81672600, 81722032, 82072916, and 91959207), the 2018 Shanghai Youth Excellent Academic Leader, the Fudan ZHUOSHI Project, the Municipal Project for Developing Emerging and Frontier Technology in Shanghai Hospitals (grant SHDC12010116), the Cooperation Project of Conquering Major Diseases in the Shanghai Municipality Health System (grant 2013ZYJB0302), the Innovation Team of the Ministry of Education (grant IRT1223), and the Shanghai Key Laboratory of Breast Cancer (grant 12DZ2260100) and the National Cancer Institute (grant P30 CA16058).
© 2021 The Author(s). Published by Elsevier Ltd.
Conflict of interest statement
The authors have declared no conflicts of interest.
Figures
References
-
- Bonadonna G., Brusamolino E., Valagussa P., Rossi A., Brugnatelli L., Brambilla C. Combination chemotherapy as an adjuvant treatment in operable breast cancer. N Engl J Med. 1976;294(8):405–410. - PubMed
-
- Early Breast Cancer Trialists' Collaborative G. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. - PubMed
-
- Early Breast Cancer Trialists' Collaborative G. Peto R., Davies C., Godwin J., Gray R., Pan H.C. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet. 2012;379(9814):432–444. - PMC - PubMed
-
- Jones S., Holmes F.A., O'Shaughnessy J., Blum J.L., Vukelja S.J., McIntyre K.J. Docetaxel with cyclophosphamide is associated with an overall survival benefit compared with Doxorubicin and Cyclophosphamide: 7-year follow-up of US oncology research trial 9735. J Clin Oncol. 2009;27(8):1177–1183. - PubMed
-
- Ejlertsen B., Tuxen M.K., Jakobsen E.H., Jensen M.B., Knoop A.S., Hojris I. Adjuvant Cyclophosphamide and Docetaxel with or without Epirubicin for early TOP2A-normal breast cancer: DBCG 07-READ, an open-label, Phase III, randomized trial. J Clin Oncol. 2017;35(23):2639–2646. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
