

The evaluation and management of patients with LDL-C ≥ 190 mg/dL in a large health care system
- PMID: 34327446
- PMCID: PMC8315478
- DOI: 10.1016/j.ajpc.2020.100002
The evaluation and management of patients with LDL-C ≥ 190 mg/dL in a large health care system
Abstract
Objectives: Patients with severe hyperlipidemia (low-density lipoprotein-cholesterol (LDL-C) ≥190 mg/dL) have a significantly increased risk of cardiovascular disease (CVD) and are more likely to have familial hypercholesterolemia (FH). We sought to determine how often health care providers recognize the implications of and adjust therapy for an LDL-C ≥190 mg/dL.
Methods: We conducted a retrospective review of patients with an LDL-C measurement in the medical record of a large health care system between November 2015 and June 2016. Patients were restricted to those with LDL-C ≥190 mg/dL and without secondary causes of dyslipidemia, with sensitivity analyses for those with LDL-C ≥220 mg/dL.
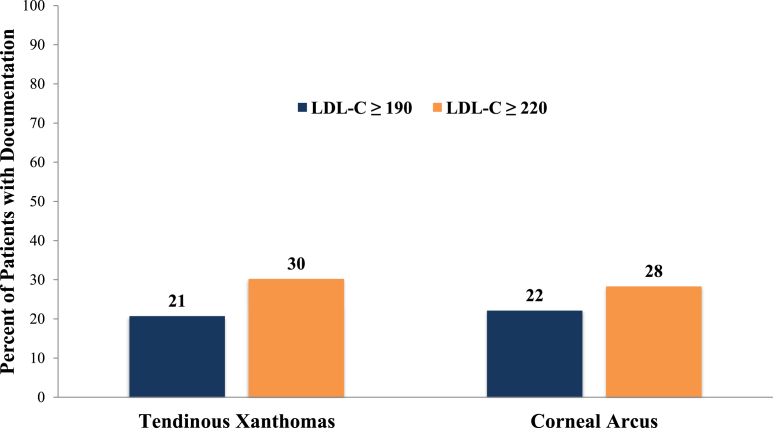
Results: Of 27,963 patients, 227 had LDL-C ≥190 mg/dL. Only 21% were on a statin at the time of LDL-C measurement. More than 90% had a follow-up clinic visit, but 41% had no change in treatment. FH was only included in the differential for 14%. The presence/absence of a family history of dyslipidemia, myocardial infarction, and premature CVD were documented in 26%, 29%, and 31%. Only 20.7% and 22.1% had documentation of the presence or absence of tendinous xanthomas or corneal arcus, respectively. Among those without prior specialist care (cardiologist or endocrinologist), only 13% were referred. These measures were only slightly better for those with LDL-C ≥220 mg/dL.
Conclusion: In a large health care system, the possibility of FH was rarely acknowledged in those with residual LDL-C ≥190 mg/dL, few were referred to specialists, and therapeutic adjustments were suboptimal. Additional efforts are required to understand barriers to improving the evaluation and management of patients with LDL-C ≥190 mg/dL.
Keywords: Familial hypercholesterolemia; Hyperlipidemia; Prevention.
© 2020 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Dr Ahmad reports grants from Regeneron Pharmaceuticals Inc, personal fees from Regeneron Pharmaceuticals Inc, personal fees from Amgen, personal fees from Akcea, grants from the National Institutes of Health–National Heart, Lung, and Blood Institute, and grants from the Familial Hypercholesterolemia Foundation.
Figures



References
-
- Stone N.J., Robinson J.G., Lichtenstein A.H. ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;129(25 Suppl 2):S1–S45. 2014. - PubMed
-
- Vallejo-Vaz A.J., Robertson M., Catapano A.L. Low-density lipoprotein cholesterol lowering for the primary prevention of cardiovascular disease among men with primary elevations of low-density lipoprotein cholesterol levels of 190 mg/dL or above: analyses from the WOSCOPS (west of scotland coronary prevention study) 5-year randomized trial and 20-year observational follow-up. Circulation. 2017;136(20):1878–1891. - PubMed
-
- Gidding S.S., Champagne M.A., de Ferranti S.D. The agenda for familial hypercholesterolemia: a scientific statement from the American heart association. Circulation. 2015;132(22):2167–2192. - PubMed
-
- Goldberg A.C., Hopkins P.N., Toth P.P. Familial hypercholesterolemia: screening, diagnosis and management of pediatric and adult patients: clinical guidance from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J Clin Lipidol. 2011;5(3 Suppl):S1–S8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
