

Early Rhythm Control Therapy in Patients With Atrial Fibrillation and Heart Failure
- PMID: 34328366
- PMCID: PMC8456351
- DOI: 10.1161/CIRCULATIONAHA.121.056323
Early Rhythm Control Therapy in Patients With Atrial Fibrillation and Heart Failure
Abstract
Background: Even on optimal therapy, many patients with heart failure and atrial fibrillation experience cardiovascular complications. Additional treatments are needed to reduce these events, especially in patients with heart failure and preserved left ventricular ejection fraction.
Methods: This prespecified subanalysis of the randomized EAST-AFNET4 trial (Early Treatment of Atrial Fibrillation for Stroke Prevention Trial) assessed the effect of systematic, early rhythm control therapy (ERC; using antiarrhythmic drugs or catheter ablation) compared with usual care (allowing rhythm control therapy to improve symptoms) on the 2 primary outcomes of the trial and on selected secondary outcomes in patients with heart failure, defined as heart failure symptoms New York Heart Association II to III or left ventricular ejection fraction [LVEF] <50%.
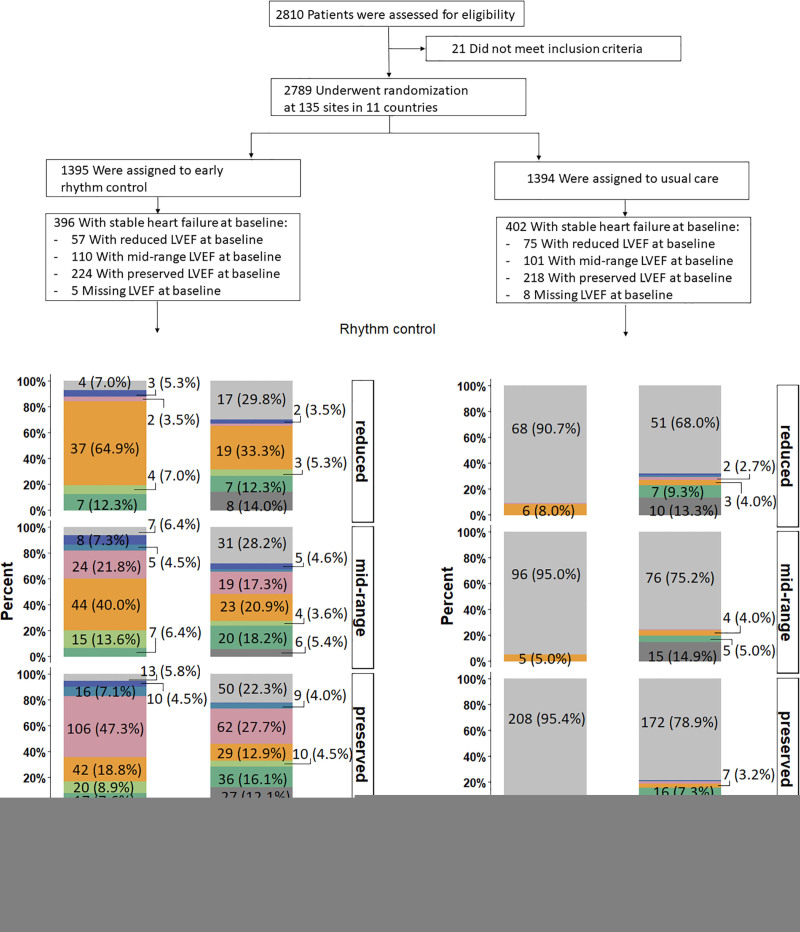
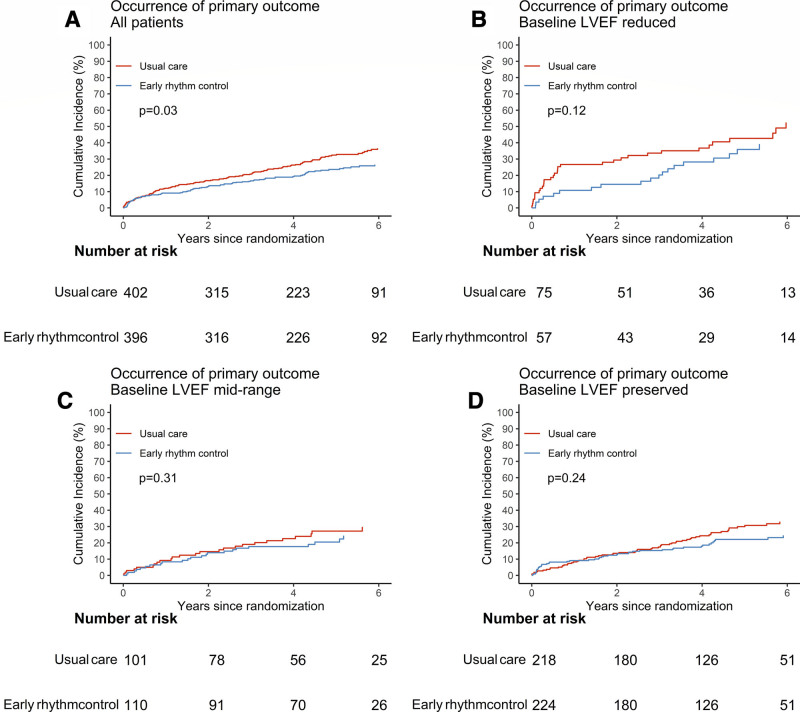
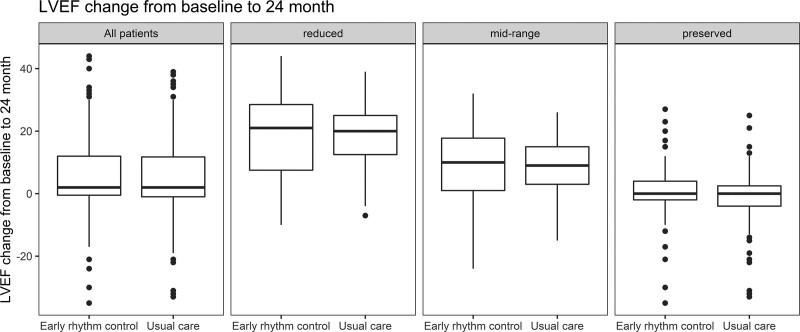
Results: This analysis included 798 patients (300 [37.6%] female, median age 71.0 [64.0, 76.0] years, 785 with known LVEF). The majority of patients (n=442) had heart failure and preserved LVEF (LVEF≥50%; mean LVEF 61±6.3%), the others had heart failure with midrange ejection fraction (n=211; LVEF 40%-49%; mean LVEF 44 ± 2.9%) or heart failure with reduced ejection fraction (n=132; LVEF<40%; mean LVEF 31±5.5%). Over the 5.1-year median follow-up, the composite primary outcome of cardiovascular death, stroke, or hospitalization for worsening of heart failure or for acute coronary syndrome occurred less often in patients randomly assigned to ERC (94/396; 5.7 per 100 patient-years) compared with patients randomly assigned to usual care (130/402; 7.9 per 100 patient-years; hazard ratio, 0.74 [0.56-0.97]; P=0.03), not altered by heart failure status (interaction P value=0.63). The primary safety outcome (death, stroke, or serious adverse events related to rhythm control therapy) occurred in 71 of 396 (17.9%) patients with heart failure randomly assigned to ERC and in 87 of 402 (21.6%) patients with heart failure randomly assigned to usual care (hazard ratio, 0.85 [0.62-1.17]; P=0.33). LVEF improved in both groups (LVEF change at 2 years: ERC 5.3±11.6%, usual care 4.9±11.6%, P=0.43). ERC also improved the composite outcome of death or hospitalization for worsening of heart failure.
Conclusions: Rhythm control therapy conveys clinical benefit when initiated within 1 year of diagnosing atrial fibrillation in patients with signs or symptoms of heart failure. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01288352. URL: http://www.controlled-trials.com; Unique identifier: ISRCTN04708680. URL: https://www.clinicaltrialsregister.eu; Unique identifier: 2010-021258-20.
Keywords: acute coronary syndrome; anti-arrhythmia agents; atrial fibrillation; atrial fibrillation ablation; controlled clinical trial; death; heart failure; stroke.
Figures
References
-
- Braunwald E. Shattuck lecture–cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. doi: 10.1056/NEJM199711063371906 - PubMed
-
- Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, Ellinor PT, Cheng S, Vasan RS, Lee DS, et al. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016;133:484–492. doi: 10.1161/CIRCULATIONAHA.115.018614 - PMC - PubMed
-
- Fabritz L, Crijns HJGM, Guasch E, Goette A, Häusler KG, Kotecha D, Lewalter T, Meyer C, Potpara TS, et al. Dynamic risk assessment to improve quality of care in patients with atrial fibrillation: the 7th AFNET/EHRA Consensus Conference. Europace. 2021;23:329–344. doi: 10.1093/europace/euaa279 - PubMed
-
- Chua W, Purmah Y, Cardoso VR, Gkoutos GV, Tull SP, Neculau G, Thomas MR, Kotecha D, Lip GYH, Kirchhof P, et al. Data-driven discovery and validation of circulating blood-based biomarkers associated with prevalent atrial fibrillation. Eur Heart J. 2019;40:1268–1276. doi: 10.1093/eurheartj/ehy815 - PMC - PubMed
-
- Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, D’Agostino RB, Murabito JM, Kannel WB, Benjamin EJ. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107:2920–2925. doi: 10.1161/01.CIR.0000072767.89944.6E - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
