

Identifying Safety Thresholds for Immunosuppressive Drugs: Applying Insights from Primary Antibody Deficiencies to Mitigate Adverse Events in Secondary Antibody Deficiencies Using Mathematical Modeling of Preclinical and Early Clinical Data
- PMID: 34328632
- PMCID: PMC8478771
- DOI: 10.1007/s13318-021-00706-z
Identifying Safety Thresholds for Immunosuppressive Drugs: Applying Insights from Primary Antibody Deficiencies to Mitigate Adverse Events in Secondary Antibody Deficiencies Using Mathematical Modeling of Preclinical and Early Clinical Data
Erratum in
-
Correction to: Identifying Safety Thresholds for Immunosuppressive Drugs: Applying Insights from Primary Antibody Deficiencies to Mitigate Adverse Events in Secondary Antibody Deficiencies Using Mathematical Modeling of Preclinical and Early Clinical Data.Eur J Drug Metab Pharmacokinet. 2021 Nov;46(6):827. doi: 10.1007/s13318-021-00719-8. Eur J Drug Metab Pharmacokinet. 2021. PMID: 34581976 Free PMC article. No abstract available.
Abstract
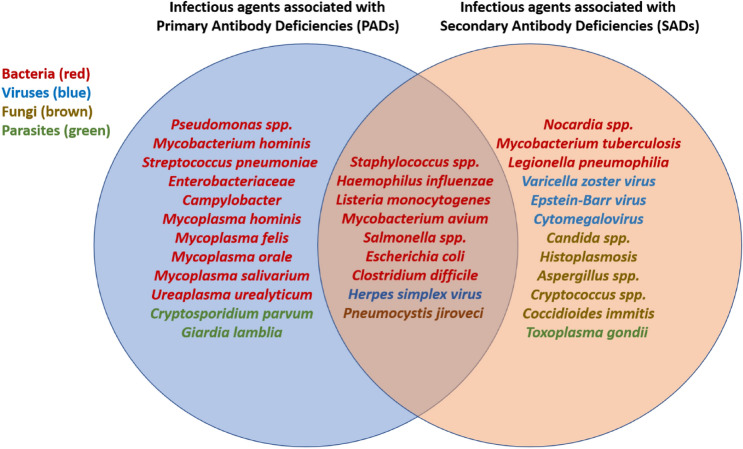
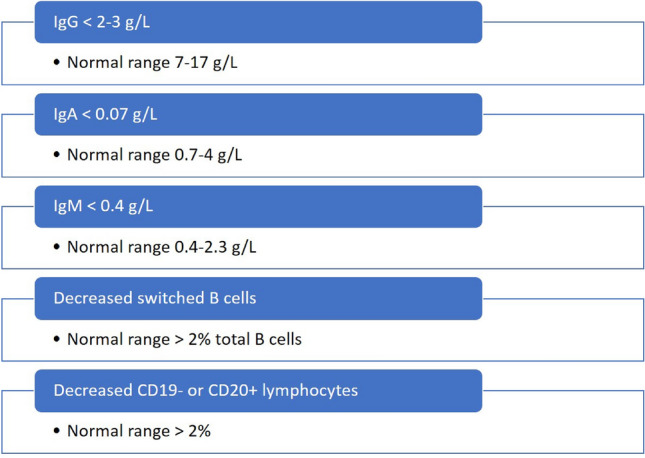
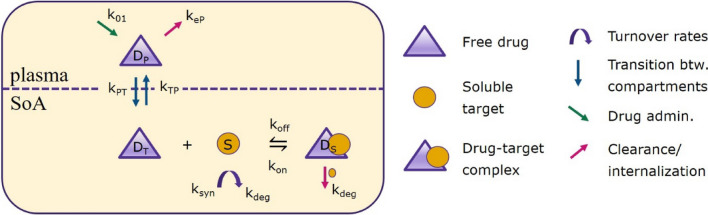
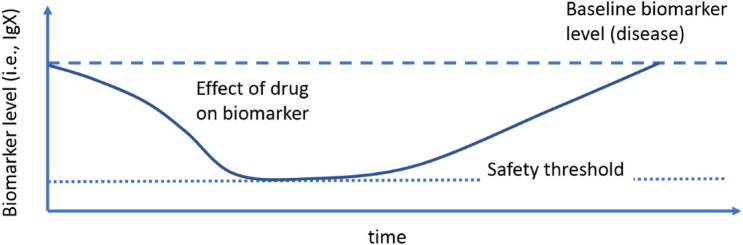
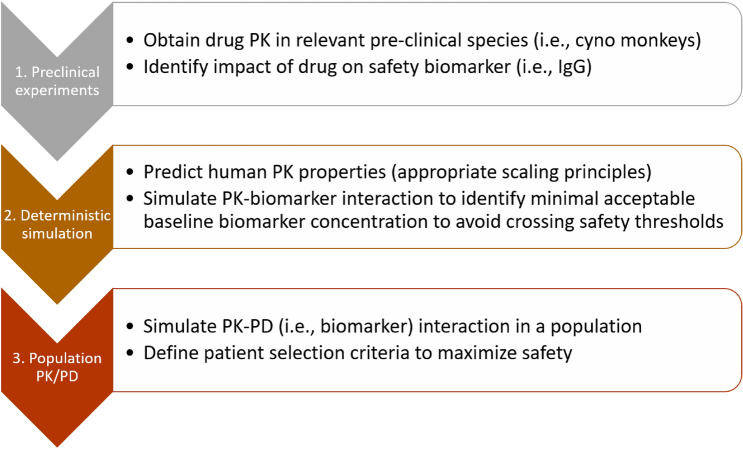
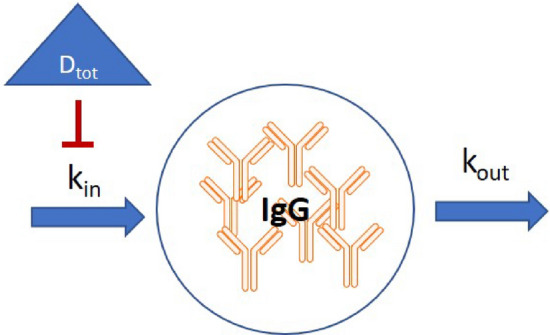
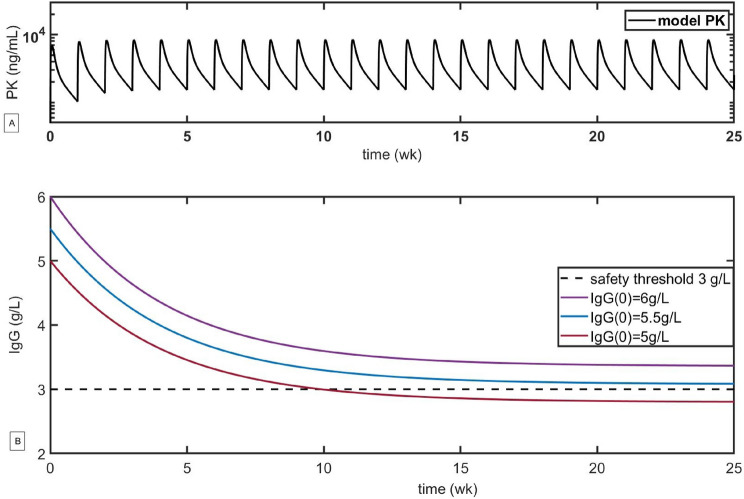
Immunosuppressive drugs can alleviate debilitating symptoms of autoimmune diseases, but, by the same token, excessive immune suppression can result in an increased risk of infection. Despite the dangers of a compromised immune system, clear definitions of what constitutes excessive suppression remain elusive. Here we review the most common infections associated with primary antibody deficiencies (PADs), such as agammaglobulinemia, common variable immunodeficiency (CVID), and IgA deficiency, as well as infections that are associated with drug-induced or secondary antibody immunodeficiencies (SADs). We identify a number of bacterial, viral, and fungal infections (e.g., Listeria monocytogenes, Staphylococcus sp., Salmonella spp., Escherichia coli, influenza, varicella zoster virus, and herpes simplex virus) associated with both PADs and SADs, and suggest that diagnostic criteria for PADs could be used as a first-line measure to identify potentially unsafe levels of immune suppression in SADs. Specifically, we suggest that, based on PAD diagnostic criteria, IgG levels should remain above 2-3 g/L, IgA levels should not fall below 0.07 g/L, and IgM levels should remain above 0.4 g/L to prevent immunosuppressive drugs from inducing mimicking PAD-like effects. We suggest that these criteria could be used in the early stages of drug development, and that pharmacokinetic and pharmacodynamic modeling could help guide patient selection to potentially improve drug safety. We illustrate the proposed approach using atacicept as an example and conclude with a discussion of the applicability of this approach for other drugs that may induce excessive immune suppression.
© 2021. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
The authors are employees of EMD Serono Research and Development Institute, Inc., a business of Merck KGaA, Darmstadt, Germany. In 2020 Merck out-licensed atacicept to Vera Therapeutics.
Figures

References
-
- Morand EF, Furie R, Tanaka Y, Bruce IN, Askanase AD, Richez C, et al. Trial of anifrolumab in active systemic lupus erythematosus. NEJM Mass Med Soc. 2020;382(3):211–221. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
