

Risk of Healthcare-Associated Transmission of Sever Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Hospitalized Cancer Patients
- PMID: 34329418
- PMCID: PMC8385815
- DOI: 10.1093/cid/ciab670
Risk of Healthcare-Associated Transmission of Sever Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in Hospitalized Cancer Patients
Abstract
Background: There is limited information on the risk of hospital-acquired coronavirus disease 2019 (COVID-19) among high-risk hospitalized patients after exposure to an infected patient or healthcare worker (HCW) in a nonoutbreak setting.
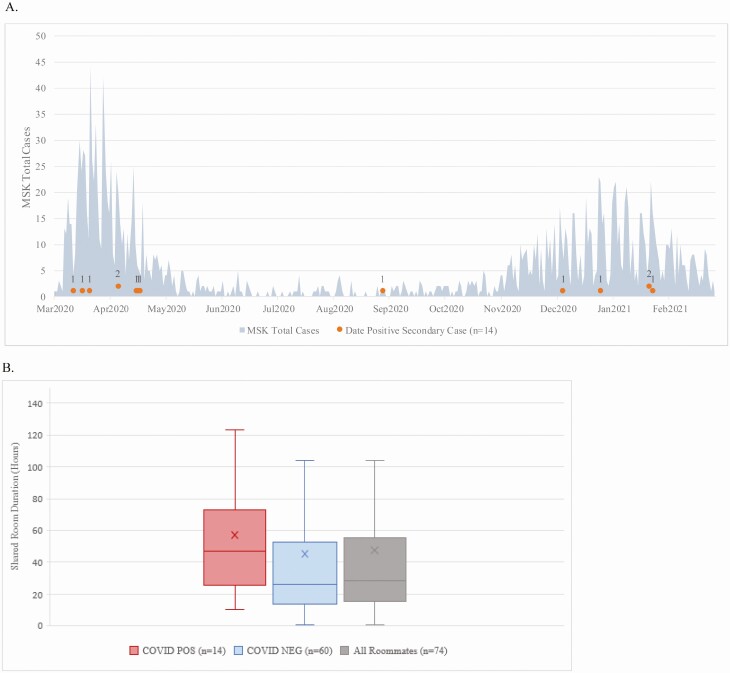
Methods: This study was conducted at a tertiary care cancer center in New York City from 10 March 2020 until 28 February 2021. In early April 2020, the study institution implemented universal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing at admission and retesting every 3 days through the hospital stay. Contact tracing records were reviewed for all exposures to SARS-CoV-2 positive patients and HCWs.
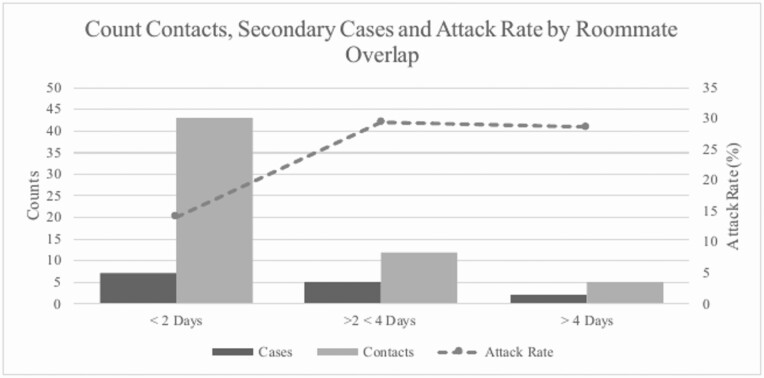
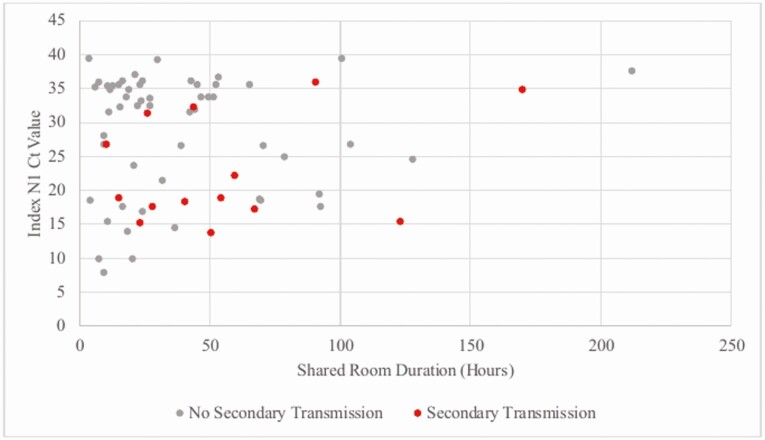
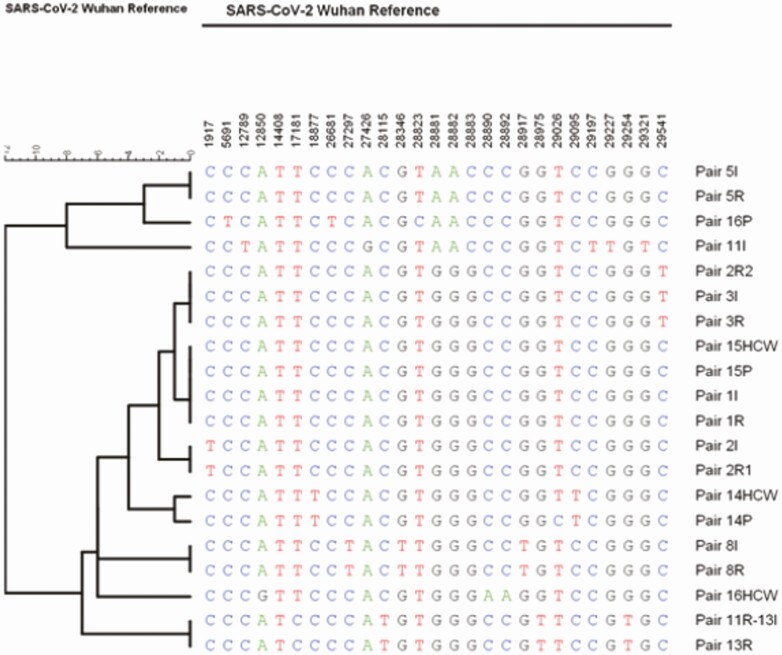
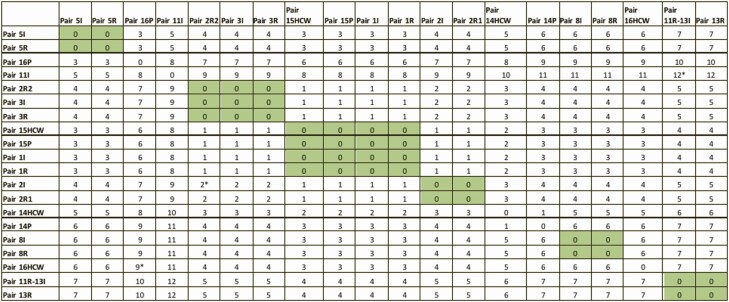
Results: From 10 March 2020 to 28 February 2021, 11 348 unique patients who were SARS-CoV-2 polymerase chain reaction (PCR) negative at the time of admission underwent 31 662 postadmission tests during their hospitalization, and 112 tested positive (0.98%). Among these, 49 patients housed in semiprivate rooms during admission resulted in 74 close contacts and 14 secondary infections within 14 days, for an overall attack rate of 18.9%. Among those exposed to a roommate undergoing an aerosol-generating procedure (AGP), the attack rate was 35.7%. Whole genome sequencing (WGS) corroborated transmission in 6/8 evaluated pairs. In addition, three transmission events occurred in 214 patients with significant exposure to 105 COVID-19 positive healthcare workers (1.4%).
Conclusions: The overall risk of hospital-acquired COVID-19 is low for hospitalized cancer patients, even during periods of high community prevalence. However, shared occupancy with an unrecognized case is associated with a high secondary attack rate in exposed roommates.
Keywords: COVID-19; SARS-CoV-2; cancer; hospital-acquired.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Centers for Disease Control and Prevention . Overview of testing for SARS-CoV-2. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-overview.html. Accessed 21 April 2021.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
