

Chronotype: what role in the context of gastroenteropancreatic neuroendocrine tumors?
- PMID: 34330303
- PMCID: PMC8325322
- DOI: 10.1186/s12967-021-03010-1
Chronotype: what role in the context of gastroenteropancreatic neuroendocrine tumors?
Abstract
Background: Chronotype is defined as a trait determining the subject circadian preference in behavioral and biological rhythms relative to external light-dark cycle. Although individual differences in chronotype have been associated with an increased risk of developing some types of cancer, no studies have been carried out in gastroenteropancreatic neuroendocrine tumors (GEP-NET).
Materials: We investigate the differences in chronotype between 109 GEP-NET and 109 healthy subjects, gender-, age-, and BMI-matched; and its correlation with tumor aggressiveness.
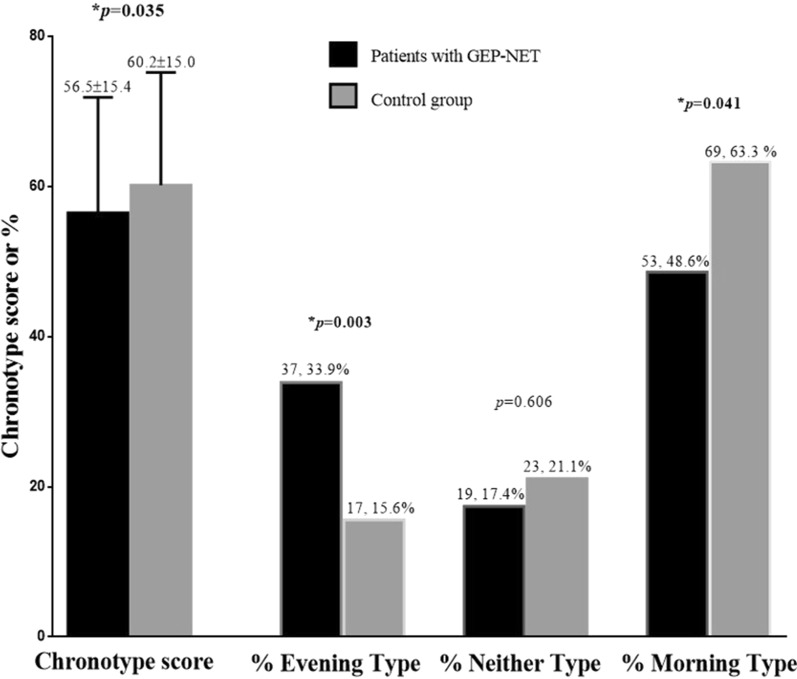
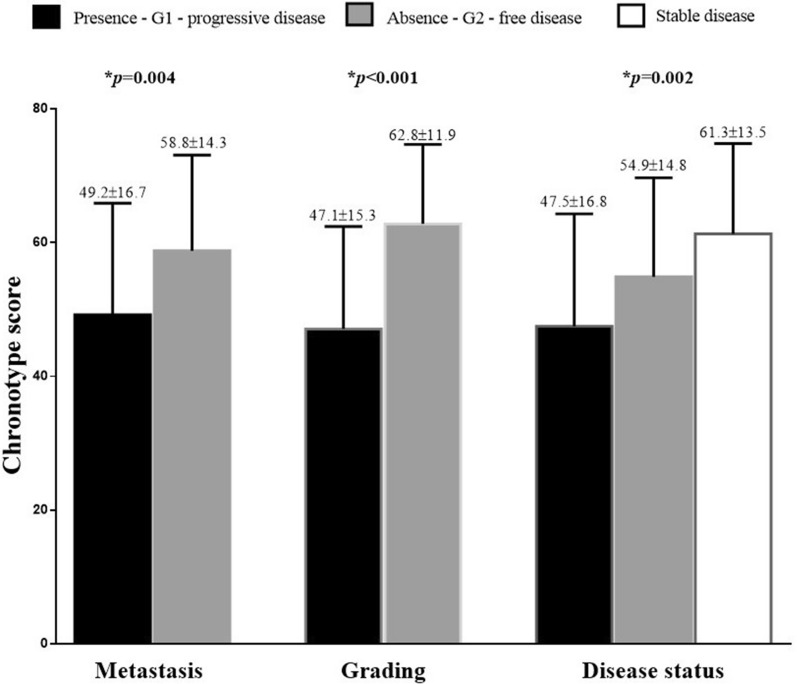
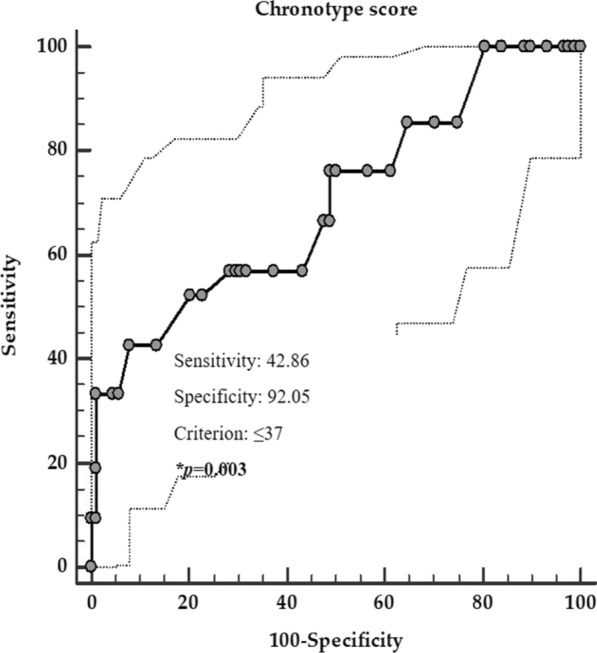
Results: GEP-NET patients have a lower chronotype score (p = 0.035) and a higher percentage of evening chronotype (p = 0.003) than controls. GEP-NET patients with morning chronotype had lower BMI, waist circumference, and higher percentage of MetS (p < 0.001) than evening type. Interestingly, considering the clinical pathological characteristics, patients with the presence of metastasis, grading G2, and in progressive disease presented the lower chronotype score (p = 0.004, p < 0.001, and p = 0.002; respectively) compared to other categories. Chronotype score was negatively associated with anthropometric measurements, metabolic profile, percentage of MetS, and Ki67 index (p < 0.001 for all).
Conclusions: GEP-NET patients have an unhealthy metabolic profile and present more commonly an evening chronotype. These results support the importance of including the assessment of chronotype in an adjunctive tool for the prevention of metabolic alterations and tumor aggressiveness of GEP-NET.
Keywords: Chronotype; Diet; Gastroenteropancreatic tumors (GEP-NET); Metabolic syndrome (MetS); Nutrition; Nutritionist; Tumor aggressiveness.
© 2021. The Author(s).
Conflict of interest statement
None of the authors have conflicts of interest to declare.
Figures
References
-
- Alexandraki KI, Tsoli M, Kyriakopoulos G, Angelousi A, Nikolopoulos G, Kolomodi D, et al. Current concepts in the diagnosis and management of neuroendocrine neoplasms of unknown primary origin. Minerva Endocrinol. 2019;44:378–386. - PubMed
-
- Tamagno G, Bennett A, Ivanovski I. Lights and darks of neuroendocrine tumors of the appendix. Minerva Endocrinol. 2020;45(4):381–392. - PubMed
-
- Vitale G, Barrea L, Aversa A. Neuroendocrine neoplasms: What we have learned and what the future holds in the pharmacological treatment. Minerava Medica. 2021;112(3):315–317. - PubMed
-
- Carra S, Gaudenzi G. New perspectives in neuroendocrine neoplasms research from tumor xenografts in zebrafish embryos. Minerva Endocrinol. 2020;45(4):393–4. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
