Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: a systematic review and meta-analysis
- PMID: 34330320
- PMCID: PMC8324455
- DOI: 10.1186/s13054-021-03697-0
Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: a systematic review and meta-analysis
Abstract
Background: Noninvasive respiratory support (NIRS) has been diffusely employed outside the intensive care unit (ICU) to face the high request of ventilatory support due to the massive influx of patients with acute respiratory failure (ARF) caused by coronavirus-19 disease (COVID-19). We sought to summarize the evidence on clinically relevant outcomes in COVID-19 patients supported by NIV outside the ICU.
Methods: We searched PUBMED®, EMBASE®, and the Cochrane Controlled Clinical trials register, along with medRxiv and bioRxiv repositories for pre-prints, for observational studies and randomized controlled trials, from inception to the end of February 2021. Two authors independently selected the investigations according to the following criteria: (1) observational study or randomized clinical trials enrolling ≥ 50 hospitalized patients undergoing NIRS outside the ICU, (2) laboratory-confirmed COVID-19, and (3) at least the intra-hospital mortality reported. Preferred Reporting Items for Systematic reviews and Meta-analysis guidelines were followed. Data extraction was independently performed by two authors to assess: investigation features, demographics and clinical characteristics, treatments employed, NIRS regulations, and clinical outcomes. Methodological index for nonrandomized studies tool was applied to determine the quality of the enrolled studies. The primary outcome was to assess the overall intra-hospital mortality of patients under NIRS outside the ICU. The secondary outcomes included the proportions intra-hospital mortalities of patients who underwent invasive mechanical ventilation following NIRS failure and of those with 'do-not-intubate' (DNI) orders.
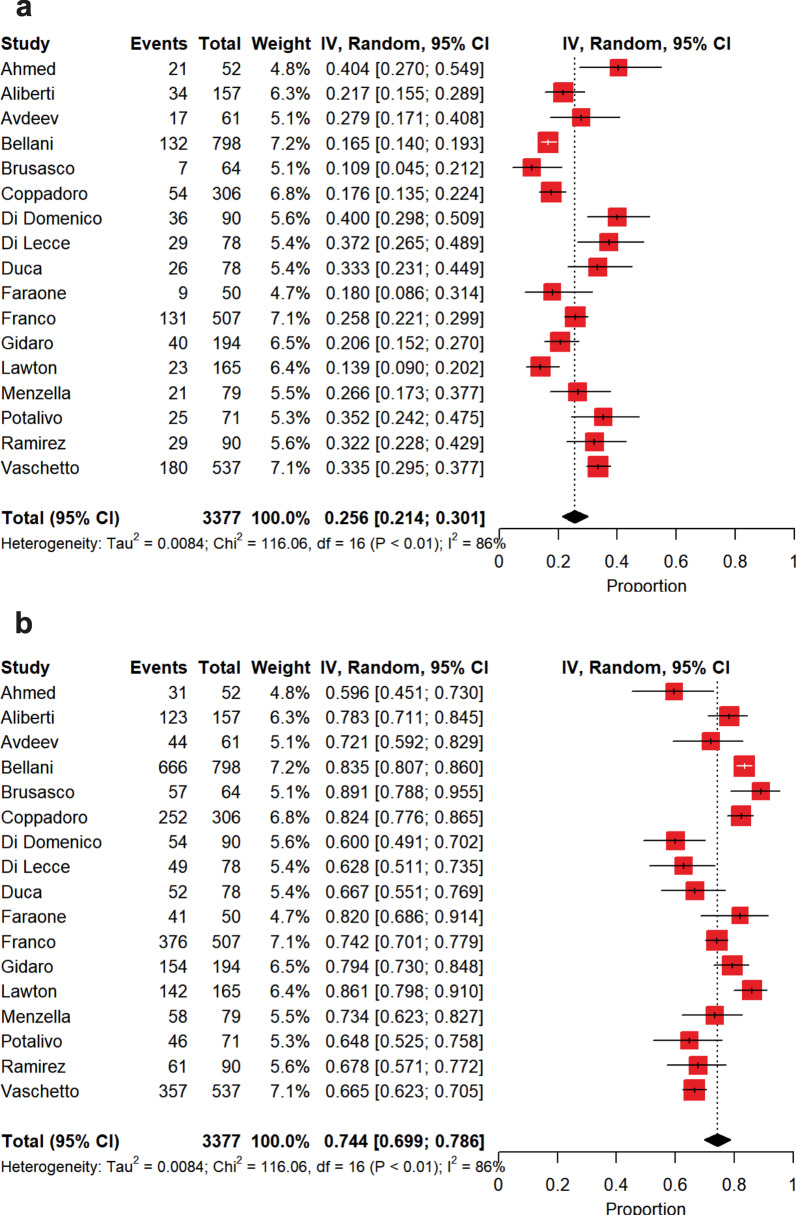
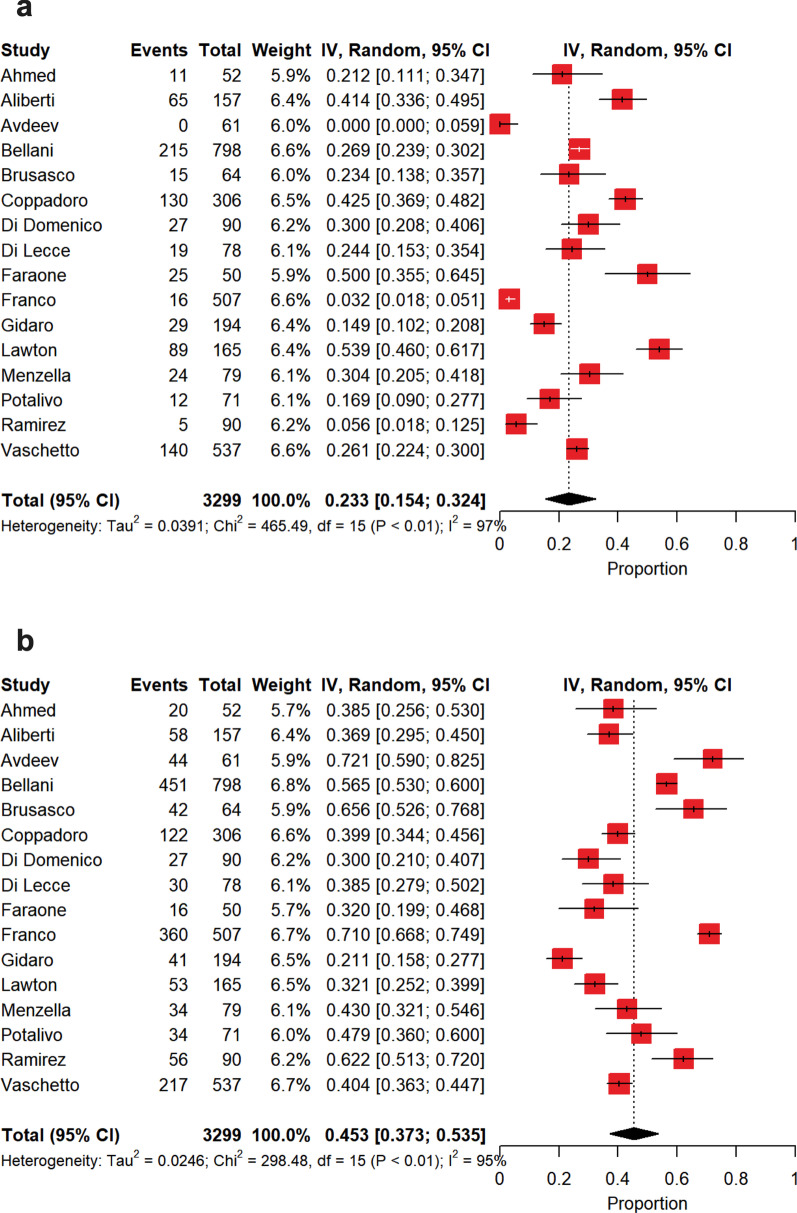
Results: Seventeen investigations (14 peer-reviewed and 3 pre-prints) were included with a low risk of bias and a high heterogeneity, for a total of 3377 patients. The overall intra-hospital mortality of patients receiving NIRS outside the ICU was 36% [30-41%]. 26% [21-30%] of the patients failed NIRS and required intubation, with an intra-hospital mortality rising to 45% [36-54%]. 23% [15-32%] of the patients received DNI orders with an intra-hospital mortality of 72% [65-78%]. Oxygenation on admission was the main source of between-study heterogeneity.
Conclusions: During COVID-19 outbreak, delivering NIRS outside the ICU revealed as a feasible strategy to cope with the massive demand of ventilatory assistance.
Registration: PROSPERO, https://www.crd.york.ac.uk/prospero/ , CRD42020224788, December 11, 2020.
Keywords: COVID-19; Intra-hospital mortality; Noninvasive ventilation.
© 2021. The Author(s).
Conflict of interest statement
The following authors declare to have no conflicts of interest: Prof Gianmaria Cammarota, Dr. Teresa Esposito, Dr. Francesco Menzella, Prof Stefano Aliberti, Dr Michele Vitacca, Prof V. Marco Ranieri, Prof Onofrio Resta, Dr Antonio Gidaro, Dr Antonella Potalivo, Dr Giuseppe Nardi, Dr Claudia Brusasco, and Prof Rosanna Vaschetto. Dr. Roberto Cosentini reports personal fees from Fisher & Paykel, outside the submitted work. Prof. Giuseppe Foti declares conference fees from DIMAR. Dr. Andrea Coppadoro has a patent and received consultancy fees from Flowmeter. Prof. Giacomo Grasselli declares personal fees (payment for lectures) from Getinge, Biotest, Draeger Medical, MSD, Fisher&Paykel; travel/accommodation/congress registration support from Biotes and Getinge; unrestricted research grant from Fisher&Paykel, MSD all outside the submitted work. Prof. Giacomo Bellani reports personal fees from Dimar and Intersurgical and is owner of a patent potentially related to this manuscript, personal fees from Draeger, Getinge, Hamilton, GE Healthcare not related to this work. Prof. Maurizio Cecconi reported personal fees from Edwards Lifesciences, Directed Systems, and Cheetah Medical outside the submitted work. Prof. Antonio Pesenti reports personal fees from Maquet, Xenios, Baxter, and Boehringer Ingelheim, outside the submitted work. Dr. Sandro Luigi Di Domenico declares relationship with Menarini group on behalf of Dynamicon education s.r.l. Dr. Tom Lawton is involved in the development of an open-source CPAP device for use in low-income countries under an EPSRC grant (no funding received). Prof. Paolo Navalesi declares to have received: grants, personal fees, and nonfinancial support from Maquet Critical Care; grants and nonfinancial support from Draeger and Intersurgical S.p.A; and personal fees from Oriopharma, Philips, Resmed, MSD, and Novartis, in each case for reasons that remain unrelated to the submitted work. Prof. Navalesi also contributed to the development of the patented ‘helmet Next,’ the royalties for which are paid to Intersurgical Spa. Prof. Navalesi contributed to the development of a device not discussed in the present study with patent application number: EP20170199831. Dr. Simonetta Tesoro received conference fees from MSD. Prof. Edoardo De Robertis received conference fees from MSD and Baxter.
Figures