

Management of gout in chronic kidney disease: a G-CAN Consensus Statement on the research priorities
- PMID: 34331037
- PMCID: PMC8458096
- DOI: 10.1038/s41584-021-00657-4
Management of gout in chronic kidney disease: a G-CAN Consensus Statement on the research priorities
Abstract
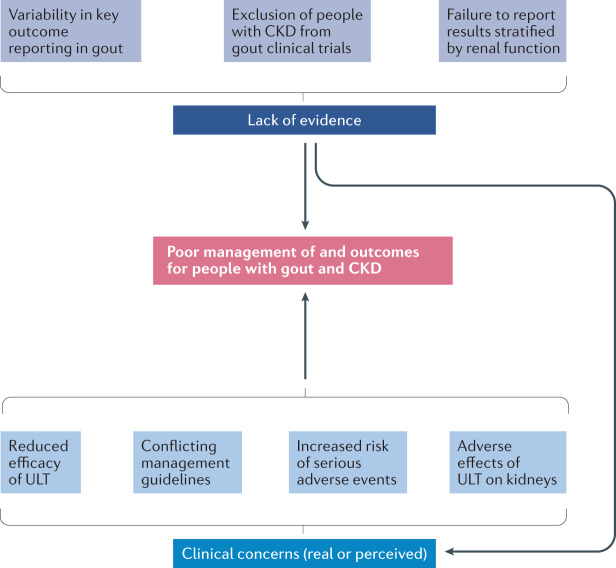
Gout and chronic kidney disease (CKD) frequently coexist, but quality evidence to guide gout management in people with CKD is lacking. Use of urate-lowering therapy (ULT) in the context of advanced CKD varies greatly, and professional bodies have issued conflicting recommendations regarding the treatment of gout in people with concomitant CKD. As a result, confusion exists among medical professionals about the appropriate management of people with gout and CKD. This Consensus Statement from the Gout, Hyperuricemia and Crystal-Associated Disease Network (G-CAN) discusses the evidence and/or lack thereof for the management of gout in people with CKD and identifies key areas for research to address the challenges faced in the management of gout and CKD. These discussions, which address areas for research both in general as well as related to specific medications used to treat gout flares or as ULT, are supported by separately published G-CAN systematic literature reviews. This Consensus Statement is not intended as a guideline for the management of gout in CKD; rather, it analyses the available literature on the safety and efficacy of drugs used in gout management to identify important gaps in knowledge and associated areas for research.
© 2021. The Author(s).
Conflict of interest statement
H.K.C. declares that he has received consulting fees from Takeda and Selecta (less than $10,000 each), research support from Horizon on an unrelated project, and is a member of the Data Safety Monitoring Committee for the VA-CSP 594 STOP GOUT clinical trial. R.T. declares that he has received consulting fees from AstraZeneca, Genentech, Horizon, SOBI (less than $10,000 each) and Selecta (more than $10,000). The other authors declare no competing interests. G-CAN is supported at arm’s length by unrestricted by grants from pharma companies including AstraZeneca, Horizon and LG within the past 12 months. No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
