

Development of prognostic models for Health-Related Quality of Life following traumatic brain injury
- PMID: 34331197
- PMCID: PMC8847302
- DOI: 10.1007/s11136-021-02932-z
Development of prognostic models for Health-Related Quality of Life following traumatic brain injury
Abstract
Background: Traumatic brain injury (TBI) is a leading cause of impairments affecting Health-Related Quality of Life (HRQoL). We aimed to identify predictors of and develop prognostic models for HRQoL following TBI.
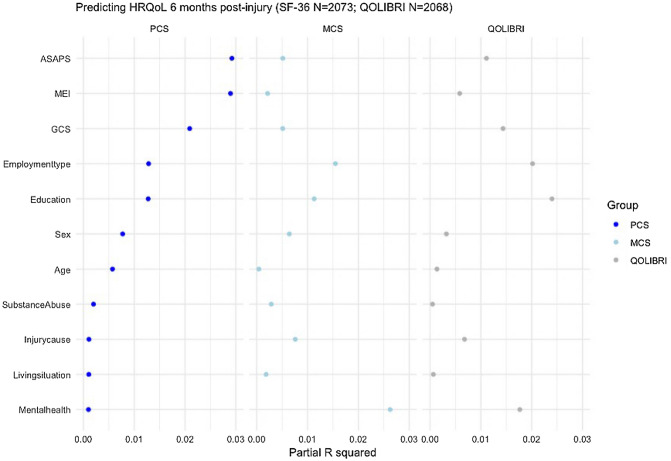
Methods: We used data from the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) Core study, including patients with a clinical diagnosis of TBI and an indication for computed tomography presenting within 24 h of injury. The primary outcome measures were the SF-36v2 physical (PCS) and mental (MCS) health component summary scores and the Quality of Life after Traumatic Brain Injury (QOLIBRI) total score 6 months post injury. We considered 16 patient and injury characteristics in linear regression analyses. Model performance was expressed as proportion of variance explained (R2) and corrected for optimism with bootstrap procedures.
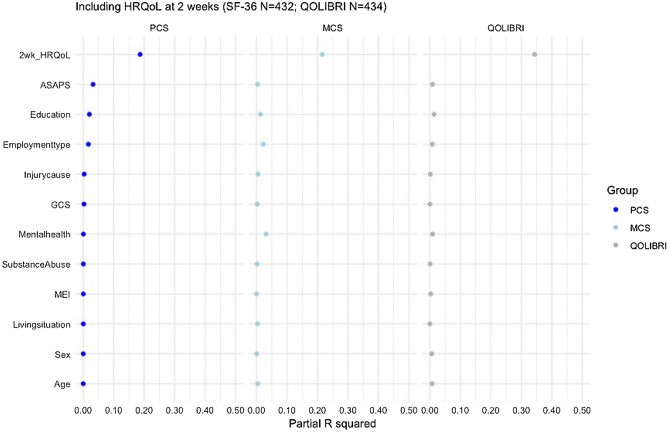
Results: 2666 Adult patients completed the HRQoL questionnaires. Most were mild TBI patients (74%). The strongest predictors for PCS were Glasgow Coma Scale, major extracranial injury, and pre-injury health status, while MCS and QOLIBRI were mainly related to pre-injury mental health problems, level of education, and type of employment. R2 of the full models was 19% for PCS, 9% for MCS, and 13% for the QOLIBRI. In a subset of patients following predominantly mild TBI (N = 436), including 2 week HRQoL assessment improved model performance substantially (R2 PCS 15% to 37%, MCS 12% to 36%, and QOLIBRI 10% to 48%).
Conclusion: Medical and injury-related characteristics are of greatest importance for the prediction of PCS, whereas patient-related characteristics are more important for the prediction of MCS and the QOLIBRI following TBI.
Keywords: Health-related quality of life; Prognostic model research; QOLIBRI; SF-36; Traumatic brain injury.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures

References
-
- Rosenfeld JV, Maas AI, Bragge P, Morganti-Kossmann MC, Manley GT, Gruen RL. Early management of severe traumatic brain injury. Lancet. 2012;9847:1088–1098. - PubMed
-
- de Koning ME, Scheenen ME, van der Horn HJ, Hageman G, Roks G, Spikman JM, van der Naalt J. Non-hospitalized patients with mild traumatic brain injury: The forgotten minority. Journal of Neurotrauma. 2017;1:257–261. - PubMed
-
- Shukla D, Devi BI, Agrawal A. Outcome measures for traumatic brain injury. Clinical Neurology and Neurosurgery. 2011;6:435–441. - PubMed
-
- Nichol AD, Higgins AM, Gabbe BJ, Murray LJ, Cooper DJ, Cameron PA. Measuring functional and quality of life outcomes following major head injury: Common scales and checklists. Injury. 2011;3:281–287. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
