

Cost-Consequence Analysis of Using Cangrelor in High Angiographic Risk Percutaneous Coronary Intervention Patients: A US Hospital Perspective
- PMID: 34331235
- PMCID: PMC8748330
- DOI: 10.1007/s40256-021-00491-9
Cost-Consequence Analysis of Using Cangrelor in High Angiographic Risk Percutaneous Coronary Intervention Patients: A US Hospital Perspective
Abstract
Objectives: The objective of this study was to evaluate a US hospital's cost implications and outcomes of cangrelor use in percutaneous coronary intervention (PCI) patients with two or more angiographic high-risk features (HRFs), including avoidance of oral P2Y12 inhibitor pretreatment in patients requiring cardiac surgery. Intravenous cangrelor provides direct, immediate onset and rapid-offset P2Y12 inhibition, which may reduce the necessity for oral P2Y12 pretreatment.
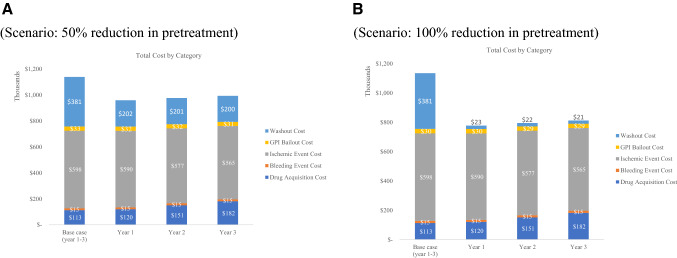
Methods: A decision analytic model was developed, estimating the annual impact over 3 years of cangrelor availability. Ischemic and bleeding events (48 h) from randomized clinical trial data were extrapolated to 30 days. Event costs were from the CHAMPION PHOENIX Economics substudy. Rates of coronary artery disease (CAD) presentation, PCI, oral P2Y12 pretreatment, and inpatient hospitalization costs were from published literature and clinical experts. Scenario analyses evaluated the impact of cangrelor availability on potential reduced P2Y12 pretreatment rates by 50-100%. Drug costs were 2019 wholesale acquisition costs and, where necessary, all costs were adjusted to 2019 dollars.
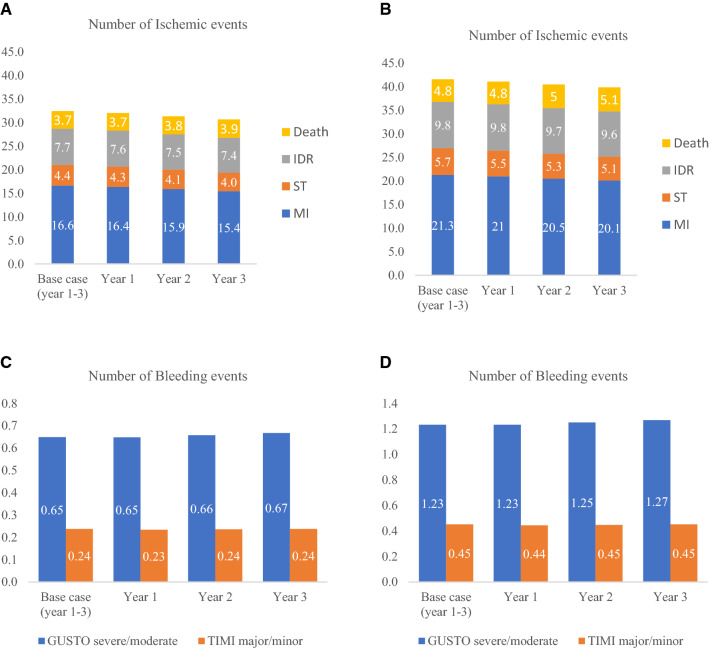
Results: In a hospital treating 1000 CAD PCI inpatients annually, increasing cangrelor use from 11 to 32% resulted in a reduction in 48-h ischemic events/year by 5.7%, while bleeding events increased by 2.9%. Total costs of $1,135,472 declined 12.8%, with a 50% reduction in P2Y12 pretreatment or 30% with no pretreatment. Savings were driven by a decrease in ischemic events, decrease in glycoprotein IIb/IIIa inhibitor use, and less need for and shorter oral P2Y12 inhibitor washout period for surgery patients.
Conclusion: Use of cangrelor in patients with two or more angiographic HRFs may improve outcomes and lower hospital budgets, mainly from avoiding surgery delays necessitated by oral P2Y12 inhibitor pretreatment.
© 2021. The Author(s).
Conflict of interest statement
Ivar S. Jensen, Elizabeth Wu, and Philip L. Cyr are employees of PrecisionHEOR, which provides consulting services to the pharmaceutical industry, including Chiesi, Inc. Marc Claussen and Khalid Salahuddin are employees of Chiesi, Inc.; Thomas Winkler was an employee of Chiesi at the time of developing this analysis; and Jayne Prats is a consultant to Chiesi, Inc. Kenneth W. Mahaffey’s financial disclosures can be viewed at
Figures


References
-
- Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58(24):e44–122. doi: 10.1016/j.jacc.2011.08.007. - DOI - PubMed
-
- Johnson TW, Mumford AD, Scott LJ, Mundell S, Butler M, Strange JW. A Study of Platelet Inhibition, Using a ‘Point of Care’ Platelet Function Test, following Primary Percutaneous Coronary Intervention for ST-Elevation Myocardial Infarction [PINPOINT-PPCI] PLoS ONE. 2015;10(12):e0144984. doi: 10.1371/journal.pone.0144984. - DOI - PMC - PubMed
-
- Kubica J, Adamski P, Ostrowska M, Sikora J, Kubica JM, Sroka WD. Morphine delays and attenuates ticagrelor exposure and action in patients with myocardial infarction: the randomized, double-blind, placebo-controlled IMPRESSION trial. Eur Heart J. 2016;37(3):245–252. doi: 10.1093/eurheartj/ehv547. - DOI - PMC - PubMed
-
- Silvain J, Storey RF, Cayla G, Esteve JB, Dillinger JG, Rousseau H. P2Y12 receptor inhibition and effect of morphine in patients undergoing primary PCI for ST-segment elevation myocardial infarction. The PRIVATE-ATLANTIC study. Thromb Haemost. 2016;116(2):369–378. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
