

Comparative Safety of Dipeptidyl Peptidase-4 Inhibitors and Sudden Cardiac Arrest and Ventricular Arrhythmia: Population-Based Cohort Studies
- PMID: 34331322
- PMCID: PMC9450482
- DOI: 10.1002/cpt.2381
Comparative Safety of Dipeptidyl Peptidase-4 Inhibitors and Sudden Cardiac Arrest and Ventricular Arrhythmia: Population-Based Cohort Studies
Abstract
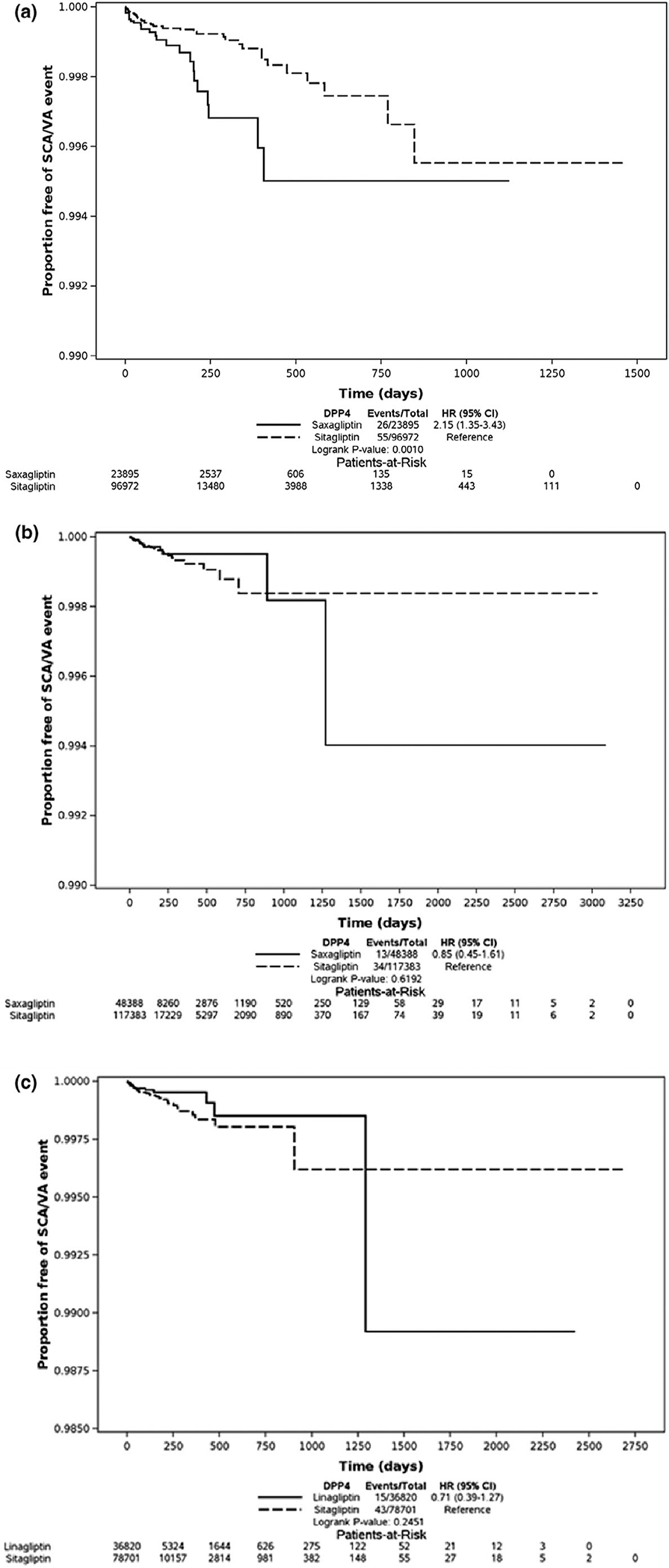
In vivo studies suggest that arrhythmia risk may be greater with less selective dipeptidyl peptidase-4 inhibitors, but evidence from population-based studies is missing. We aimed to compare saxagliptin, sitagliptin, and linagliptin with regard to risk of sudden cardiac arrest (SCA)/ventricular arrhythmia (VA). We conducted high-dimensional propensity score (hdPS) matched, new-user cohort studies. We analyzed Medicaid and Optum Clinformatics separately. We identified new users of saxagliptin, sitagliptin (both databases), and linagliptin (Optum only). We defined SCA/VA outcomes using emergency department and inpatient diagnoses. We identified and then controlled for confounders via a data-adaptive, hdPS approach. We generated marginal hazard ratios (HRs) via Cox proportional hazards regression using a robust variance estimator while adjusting for calendar year. We identified the following matched comparisons: saxagliptin vs. sitagliptin (23,895 vs. 96,972) in Medicaid, saxagliptin vs. sitagliptin (48,388 vs. 117,383) in Optum, and linagliptin vs. sitagliptin (36,820 vs. 78,701) in Optum. In Medicaid, use of saxagliptin (vs. sitagliptin) was associated with an increased rate of SCA/VA (adjusted HR (aHR), 2.01, 95% confidence interval (CI) 1.24-3.25). However, in Optum data, this finding was not present (aHR, 0.79, 95% CI 0.41-1.51). Further, we found no association between linagliptin (vs. sitagliptin) and SCA/VA (aHR, 0.65, 95% CI 0.36-1.17). We found discordant results regarding the association between SCA/VA with saxagliptin compared with sitagliptin in two independent datasets. It remains unclear whether these findings are due to heterogeneity of treatment effect in the different populations, chance, or unmeasured confounding.
© 2021 The Authors. Clinical Pharmacology & Therapeutics © 2021 American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
CONFLICT OF INTEREST
C.E.L. serves on the Executive Committee of SH directs the University of Pennsylvania’s Center for Pharmacoepidemiology Research Training. The Center receives funds for education from Pfizer Sanofi. C.E.L. has received honoraria from the University of Florida the American College of Clinical Pharmacy Foundation. C.E.L. receives travel support from John Wiley & Sons. S.H. has consulted for the Medullary Thyroid Cancer Consortium (Novo Nordisk, AstraZeneca, Eli Lilly, GlaxoSmithKline) on matters unrelated to the topic of this paper. W.B.B. has consulted for Genentech on matters unrelated to the topic of this paper. J.H.F. has consulted for Genentech, Eli Lilly, Boehringer Ingelheim on matters unrelated to the topic of this paper. S.E.K. has consulted for GlaxoSmithKline Janssen, unrelated to the contents of this study. Z.B. has consulted for Astra Zeneca, Merck, Boehringer Ingelheim, Sanofi on matters unrelated to the topic of this paper. All other authors declared no competing interests for this work.
Figures
Similar articles
-
Adherence, Persistence, and Health Care Costs for Patients Receiving Dipeptidyl Peptidase-4 Inhibitors.J Manag Care Spec Pharm. 2017 Mar;23(3):299-306. doi: 10.18553/jmcp.2017.23.3.299. J Manag Care Spec Pharm. 2017. PMID: 28230454 Free PMC article.
-
Risk for Hospitalized Heart Failure Among New Users of Saxagliptin, Sitagliptin, and Other Antihyperglycemic Drugs: A Retrospective Cohort Study.Ann Intern Med. 2016 Jun 7;164(11):705-14. doi: 10.7326/M15-2568. Epub 2016 Apr 26. Ann Intern Med. 2016. PMID: 27110660 Free PMC article.
-
The risk of sudden cardiac arrest and ventricular arrhythmia with rosiglitazone versus pioglitazone: real-world evidence on thiazolidinedione safety.Cardiovasc Diabetol. 2020 Feb 25;19(1):25. doi: 10.1186/s12933-020-00999-5. Cardiovasc Diabetol. 2020. PMID: 32098624 Free PMC article.
-
An update on the 'gliptins'.Drug Ther Bull. 2016 Dec;54(12):138-141. doi: 10.1136/dtb.2016.12.0442. Drug Ther Bull. 2016. PMID: 27979881 Review.
-
Cardiovascular events and all-cause mortality in patients with type 2 diabetes treated with dipeptidyl peptidase-4 inhibitors: An extensive meta-analysis of randomized controlled trials.Nutr Metab Cardiovasc Dis. 2021 Sep 22;31(10):2745-2755. doi: 10.1016/j.numecd.2021.06.002. Epub 2021 Jul 5. Nutr Metab Cardiovasc Dis. 2021. PMID: 34364771
Cited by
-
Associations between Oral Glucose-Lowering Agents and Increased Risk for Life-Threatening Arrhythmias in Patients with Type 2 Diabetes Mellitus-A Literature Review.Medicina (Kaunas). 2023 Oct 2;59(10):1760. doi: 10.3390/medicina59101760. Medicina (Kaunas). 2023. PMID: 37893478 Free PMC article. Review.
-
Do relationships between ambient temperature and serious adverse health outcomes vary among users of different antidiabetes drugs? A retrospective cohort study of US Medicaid beneficiaries with type 2 diabetes.BMJ Open. 2024 Oct 21;14(10):e085139. doi: 10.1136/bmjopen-2024-085139. BMJ Open. 2024. PMID: 39433419 Free PMC article.
-
Evaluating the Potential of Prevalent New User Design as an Alternative When New User Design is Impractical.Pragmat Obs Res. 2025 Jul 31;16:155-168. doi: 10.2147/POR.S517514. eCollection 2025. Pragmat Obs Res. 2025. PMID: 40765627 Free PMC article.
References
-
- Montvida O, Shaw J, Atherton JJ, Stringer F & Paul SK Long-term trends in antidiabetes drug usage in the U.S.: Real-world evidence in patients newly diagnosed with type 2 diabetes. Diabetes Care 41, 69–78 (2018). - PubMed
-
- Ahren B Dipeptidyl peptidase-4 inhibitors: Clinical data clinical implications. Diabetes Care 30, 1344–1350 (2007). - PubMed
-
- Koyani CN et al. Dipeptidyl peptidase-4 independent cardiac dysfunction links saxagliptin to heart failure. Biochem. Pharmacol. 145, 64–80 (2017). - PubMed
-
- Tang ST et al. Sitagliptin inhibits endothelin-1 expression in the aortic endothelium of rats with streptozotocin-induced diabetes by suppressing the nuclear factor-k appaB/IkappaBalpha system through the activation of AMP-activated protein kinase. Int. J. Mol. Med. 37, 1558–1566 (2016). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
