

Cardiovascular outcomes with sodium-glucose cotransporter-2 inhibitors vs other glucose-lowering drugs in 13 countries across three continents: analysis of CVD-REAL data
- PMID: 34332558
- PMCID: PMC8325810
- DOI: 10.1186/s12933-021-01345-z
Cardiovascular outcomes with sodium-glucose cotransporter-2 inhibitors vs other glucose-lowering drugs in 13 countries across three continents: analysis of CVD-REAL data
Abstract
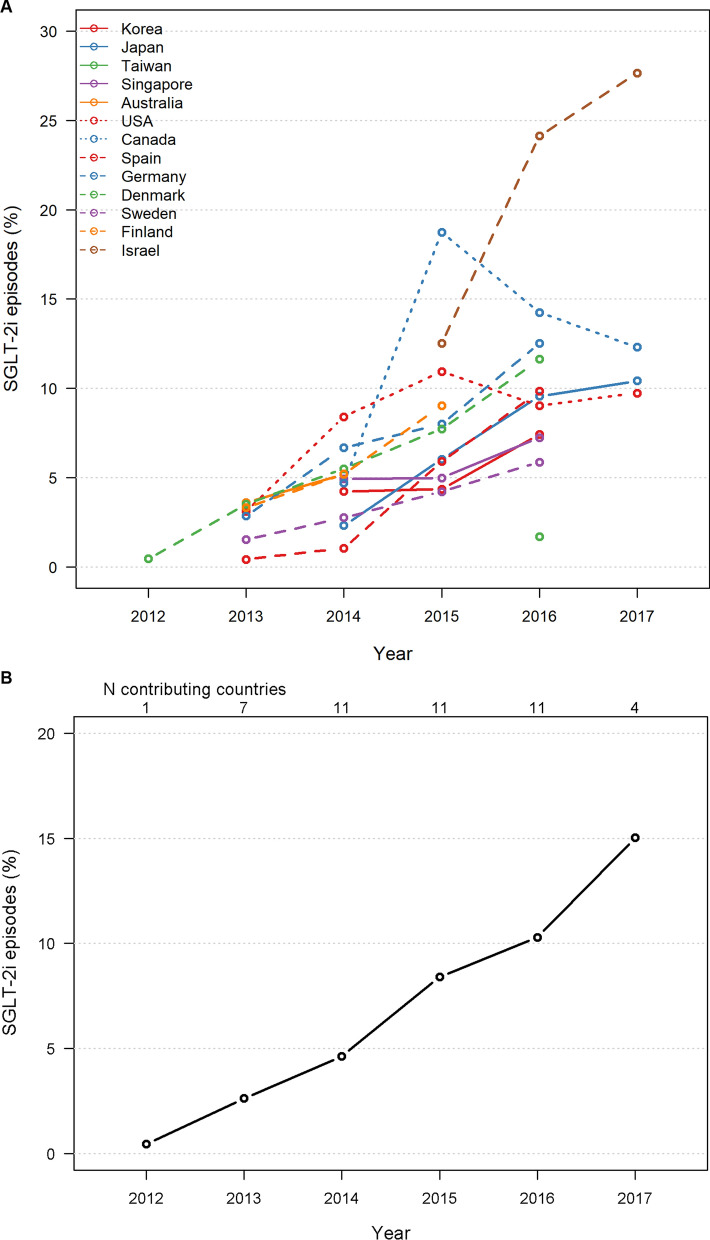
Background: Randomized, controlled cardiovascular outcome trials may not be fully representative of the management of patients with type 2 diabetes across different geographic regions. We conducted analyses of data from the multinational CVD-REAL consortium to determine the association between initiation of sodium-glucose cotransporter-2 inhibitors (SGLT-2i) and cardiovascular outcomes, including subgroup analyses based on patient characteristics.
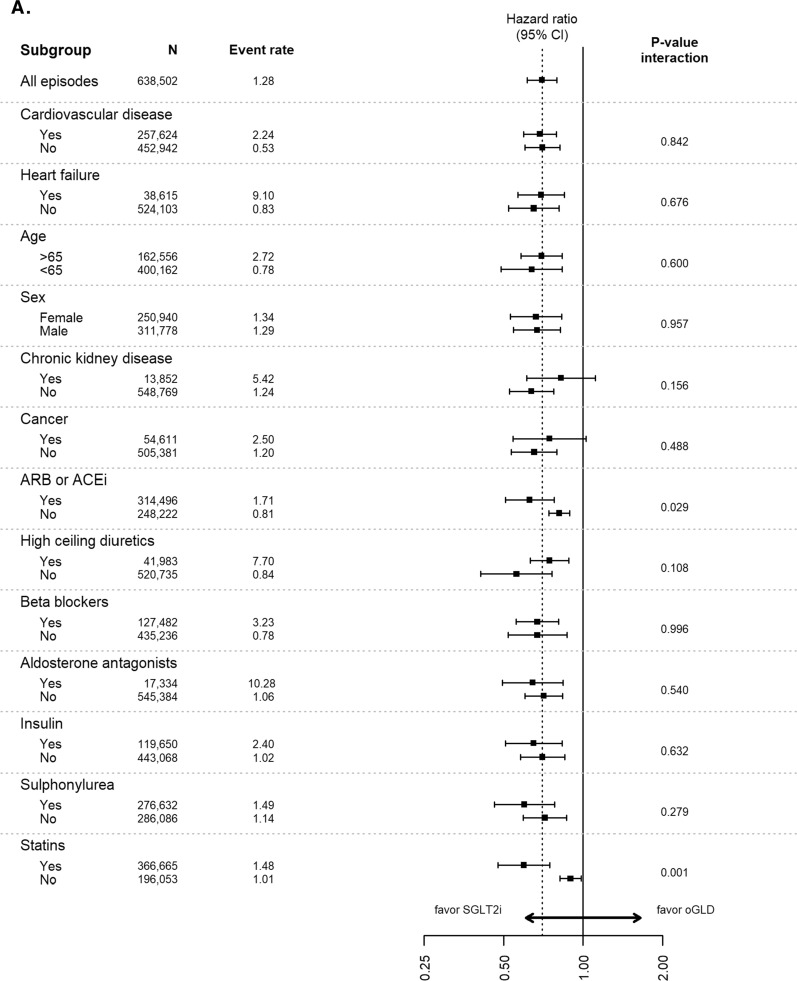
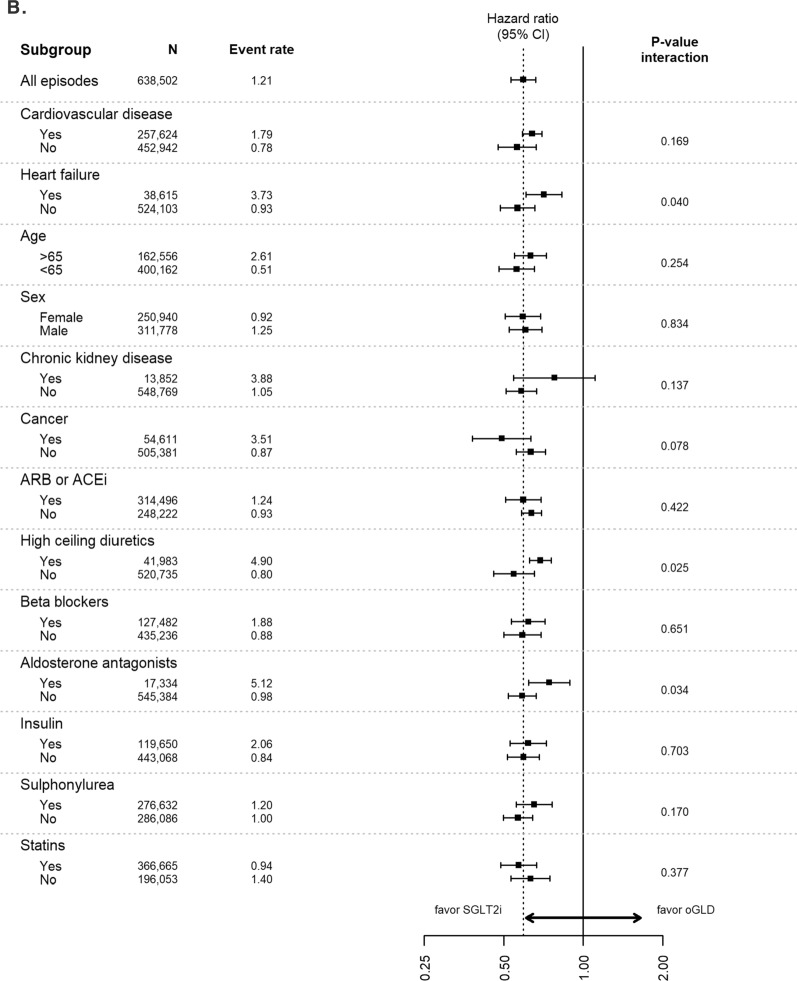
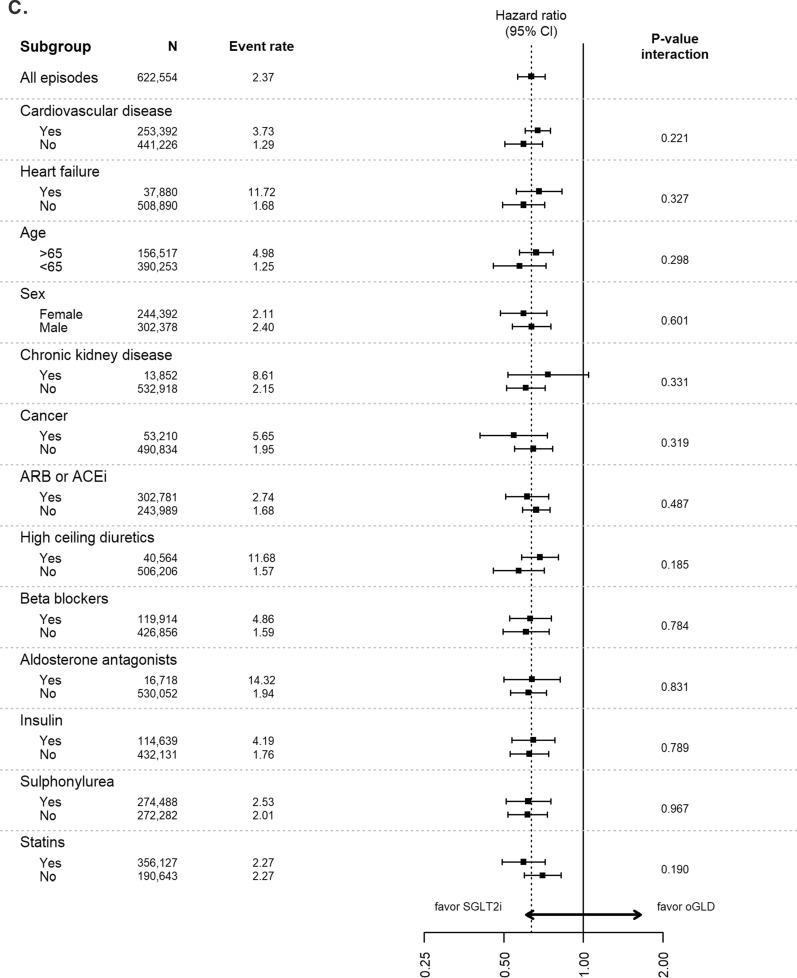
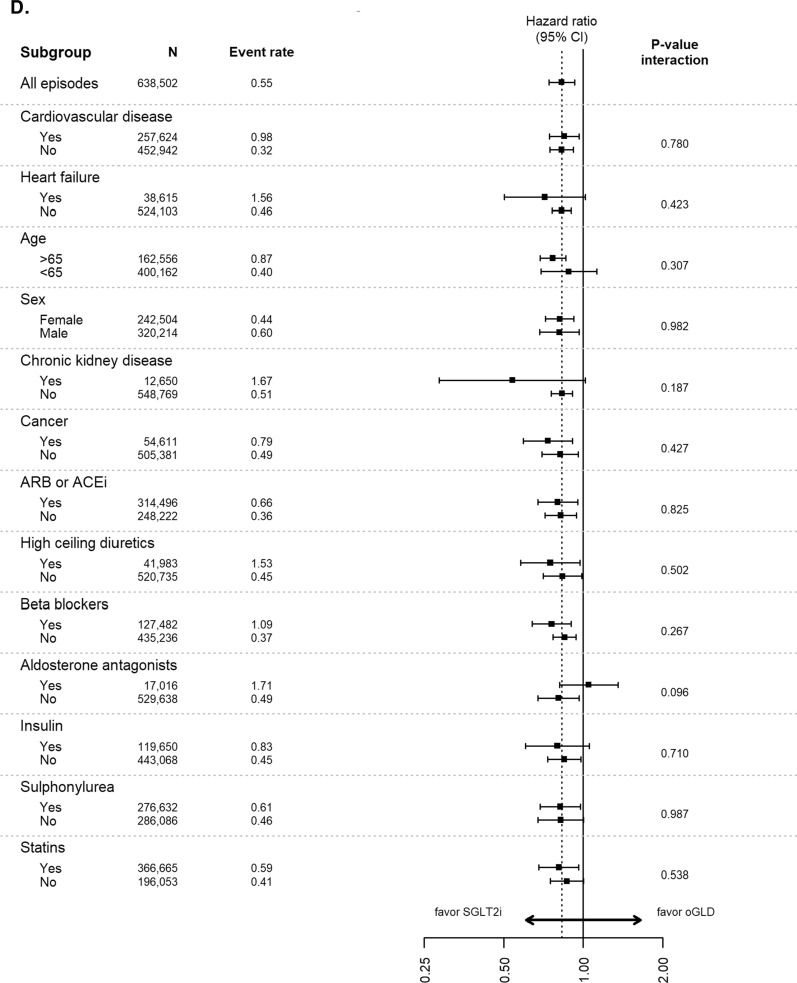
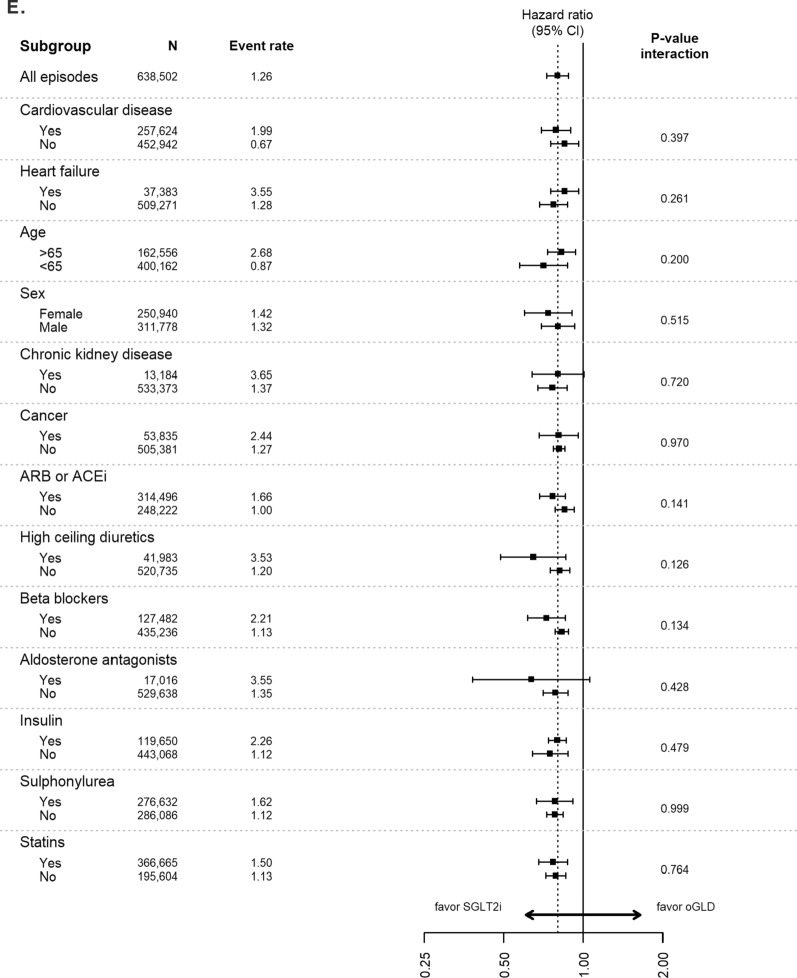
Methods: De-identified health records from 13 countries across three continents were used to identify patients newly-initiated on SGLT-2i or other glucose-lowering drugs (oGLDs). Propensity scores for SGLT-2i initiation were developed in each country, with 1:1 matching for oGLD initiation. In the matched groups hazard ratios (HRs) for hospitalization for heart failure (HHF), all-cause death (ACD), the composite of HHF or ACD, myocardial infarction (MI) and stroke were estimated by country, and pooled using a weighted meta-analysis. Multiple subgroup analyses were conducted across patient demographic and clinical characteristics to examine any heterogeneity in treatment effects.
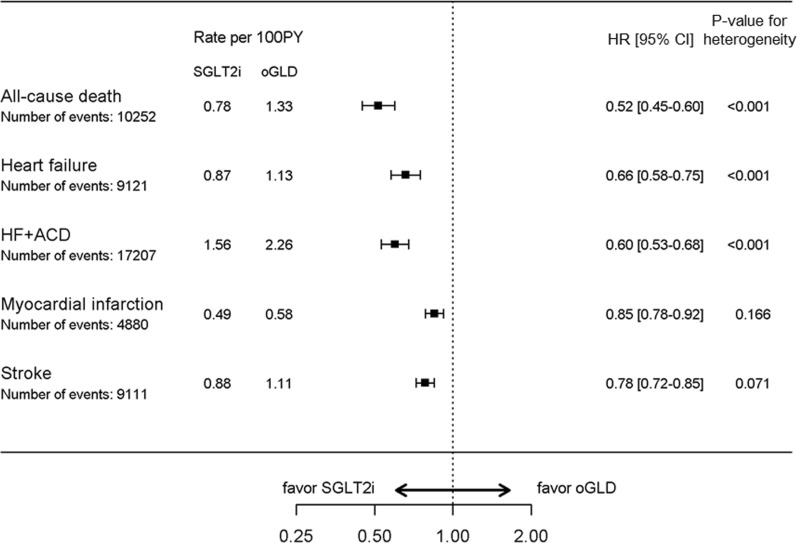
Results: Following matching, 440,599 new users of SGLT-2i and oGLDs were included in each group. Mean follow-up time was 396 days for SGLT-2i initiation and 406 days for oGLDs initiation. SGLT-2i initiation was associated with a lower risk of HHF (HR: 0.66, 95%CI 0.58-0.75; p < 0.001), ACD (HR: 0.52, 95%CI 0.45-0.60; p < 0.001), the composite of HHF or ACD (HR: 0.60, 95%CI 0.53-0.68; p < 0.001), MI (HR: 0.85, 95%CI 0.78-0.92; p < 0.001), and stroke (HR: 0.78, 95%CI 0.72-0.85; p < 0.001); regardless of patient characteristics, including established cardiovascular disease, or geographic region.
Conclusions: This CVD-REAL study extends the findings from the SGLT-2i clinical trials to the broader setting of an ethnically and geographically diverse population, and across multiple subgroups. Trial registration NCT02993614.
Keywords: Cardiovascular outcomes; Heart failure; Sodium–glucose cotransporter-2 inhibitors; Type 2 diabetes.
© 2021. The Author(s).
Conflict of interest statement
KK reports grants from AstraZeneca, during the conduct of the study; grants from Amgen, grants from AstraZeneca, grants from Bayer, grants from NAPP, grants from Lilly, from Merck Sharp & Dohme, personal fees from Novartis, personal fees from Novo Nordisk, personal fees from Roche, personal fees from Berlin-Chemie AG/Menarini Group, personal fees from Sanofi-Aventis, personal fees from Servier, personal fees from Boehringer Ingelheim, grants from Pfizer, grants from Boehringer Ingelheim, grants from AstraZeneca, grants from Novartis, grants from Novo Nordisk, grants from Sanofi-Aventis, grants from Lilly, grants from Merck Sharp & Dohme, grants from Servier, outside the submitted work.
SK has received grants from Bayer Yakuhin and Daiichi Sankyo and consulting fees from Bayer Yakuhin, Bristol-Myers Squibb, and Pfizer.
CSPL has received research support from Boston Scientific, Bayer, Roche Diagnostics, AstraZeneca, Medtronic, and Vifor Pharma; has served as consultant or on the Advisory Board/ Steering Committee/ Executive Committee for Abbott Diagnostics, Amgen, Applied Therapeutics, AstraZeneca, Bayer, Biofourmis, Boehringer Ingelheim, Boston Scientific, Corvia Medical, Cytokinetics, Darma Inc., Us2.ai, JanaCare, Janssen Research & Development LLC, Medtronic, Menarini Group, Merck, MyoKardia, Novartis, Novo Nordisk, Radcliffe Group Ltd., Roche Diagnostics, Sanofi, Stealth BioTherapeutics, The Corpus, Vifor Pharma and WebMD Global LLC; and serves as co-founder & non-executive director of Us2.ai.
MAC reports research support to his institution from Amgen, AstraZeneca, CSL Behring, GlaxoSmithKline, Novartis; consulting fees from Amgen, AstraZeneca, Bayer, Boehringer-Ingelheim, Boston Scientific, Edwards Lifesciences, Merck, Novo-Nordisk.
AN has received personal fees from AstraZeneca for this study, and honorarium for lectures and advisory board meetings for Novo Nordisk, Boehringer Ingelheim, and Lilly.
MEJ is a shareholder of Novo Nordisk. MEJ has received grants from AstraZeneca, Amgen, Boehringer Ingelheim and Sanofi Aventis.
RWH has received grants to his institution from AstraZeneca.
JF-N has received grants to his institution from AstraZeneca for this study and has received honoraria for lectures and consulting from Novartis, NovoNordisk, Sanofi, Lilly, Boehringer Ingelheim and Merck Sharp & Dohme.
NT has received consulting fees from Otsuka, Tricida, BI-Lilly, Janssen and AstraZeneca. He has received research support from AstraZeneca, Otsuka and Janssen, including for this work. He owns stock in Tricida, Pulsedata, Mesentech and Renibus. His research program is supported by the Canadian Institute for Health Research and Research Manitoba.
JES has received honoraria for advisory boards and lectures from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Mylan, Novartis, Novo Nordisk, Pfizer, and Sanofi.
AK has received grants and consulting fees from AstraZeneca, Novo Nordisk, Merck, and Boheringer Ingelheim.
S-YG has received institutional grants from AstraZeneca, Medtronic, and Sanofi. He has participated in advisory boards for Amgen, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Medtronic and Sanofi and has received honoraria for participation.
C-EC has received honorarium from AstraZeneca, Boehringer Ingelheim, Daiichi-Sankyo, MSD, Novartis, Pfizer, Sanofi.
JGE has received honorarium for lectures and advisory board meetings for Novo Nordisk, Boehringer Ingelheim, and AstraZeneca.
FZ has received honoraria for lectures from Napp Pharmaceuticals and Boehringer Ingelheim.
DM has received grants to her institution from AstraZeneca.
MT is an employee at Statisticon for which AstraZeneca is a client.
HC, EW, JS, FS and PF are AstraZeneca employees and hold stock options. JB is a AstraZeneca employee.
MK has received research grants from AstraZeneca and Boehringer Ingelheim, has served on advisory boards for AstraZeneca, Boehringer Ingelheim, Sanofi, Glytec, Novo Nordisk, ZS Pharma, Janssen, Merck (Diabetes) and Novartis; consultant for AstraZeneca, Boehringer Ingelheim, Sanofi, GSK, Janssen, Intarcia, Merck (Diabetes), Novo Nordisk, Glytec and ZS Pharma.
Figures
References
-
- Kosiborod M, Gomes MB, Nicolucci A, Pocock S, Rathmann W, Shestakova MV, et al. Vascular complications in patients with type 2 diabetes: prevalence and associated factors in 38 countries (the DISCOVER study program) Cardiovasc Diabetol. 2018;17(1):150. doi: 10.1186/s12933-018-0787-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
