

An uncommon etiological factor for aspiration pneumonitis caused by spontaneous sphenoid sinus meningoencephalocele with cerebrospinal fluid rhinorrhea: a case report
- PMID: 34332562
- PMCID: PMC8325533
- DOI: 10.1186/s12890-021-01620-5
An uncommon etiological factor for aspiration pneumonitis caused by spontaneous sphenoid sinus meningoencephalocele with cerebrospinal fluid rhinorrhea: a case report
Abstract
Background: Aspiration pneumonitis is an inflammatory disease of the lungs which is difficult to diagnose accurately. Large-volume aspiration of oropharyngeal or gastric contents is essential for the development of aspiration pneumonitis. The role of cerebrospinal fluid (CSF) rhinorrhea is often underestimated as a rare etiological factor for aspiration in the diagnosis process of aspiration pneumonitis.
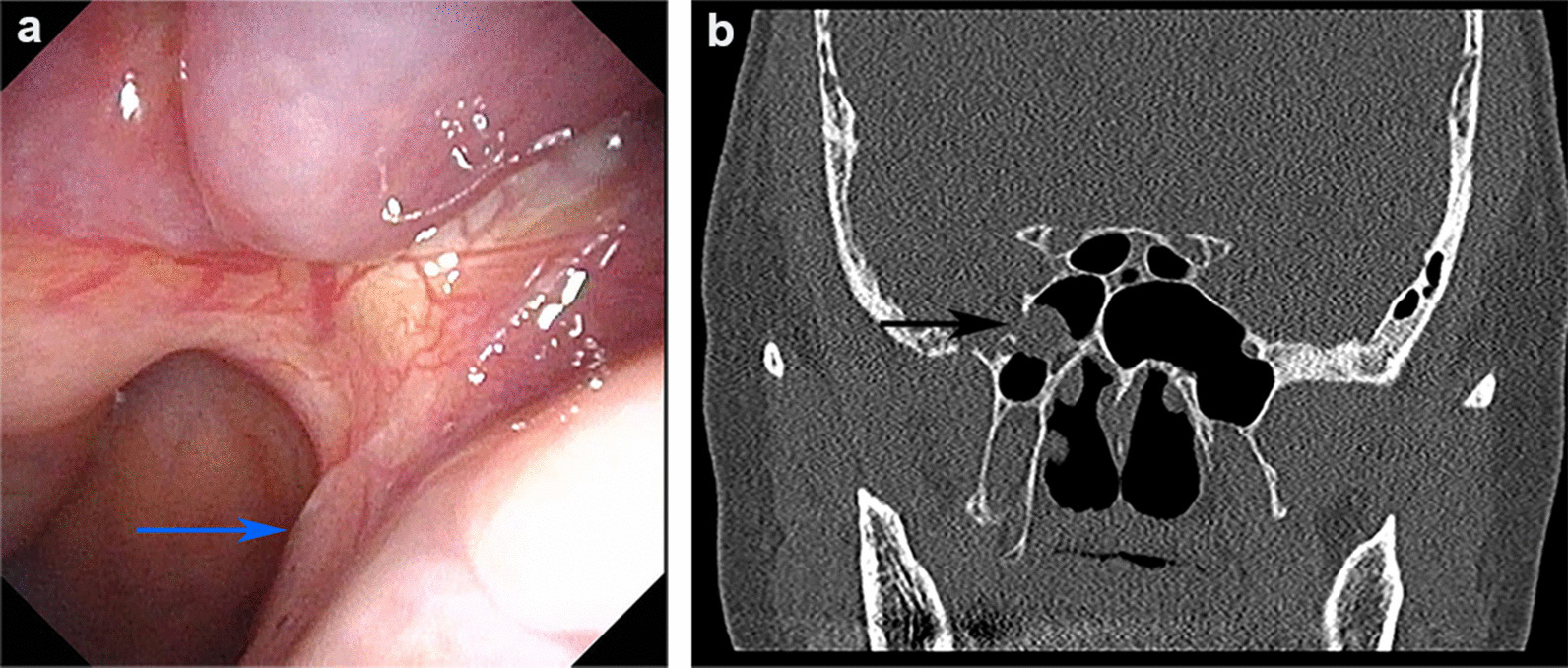
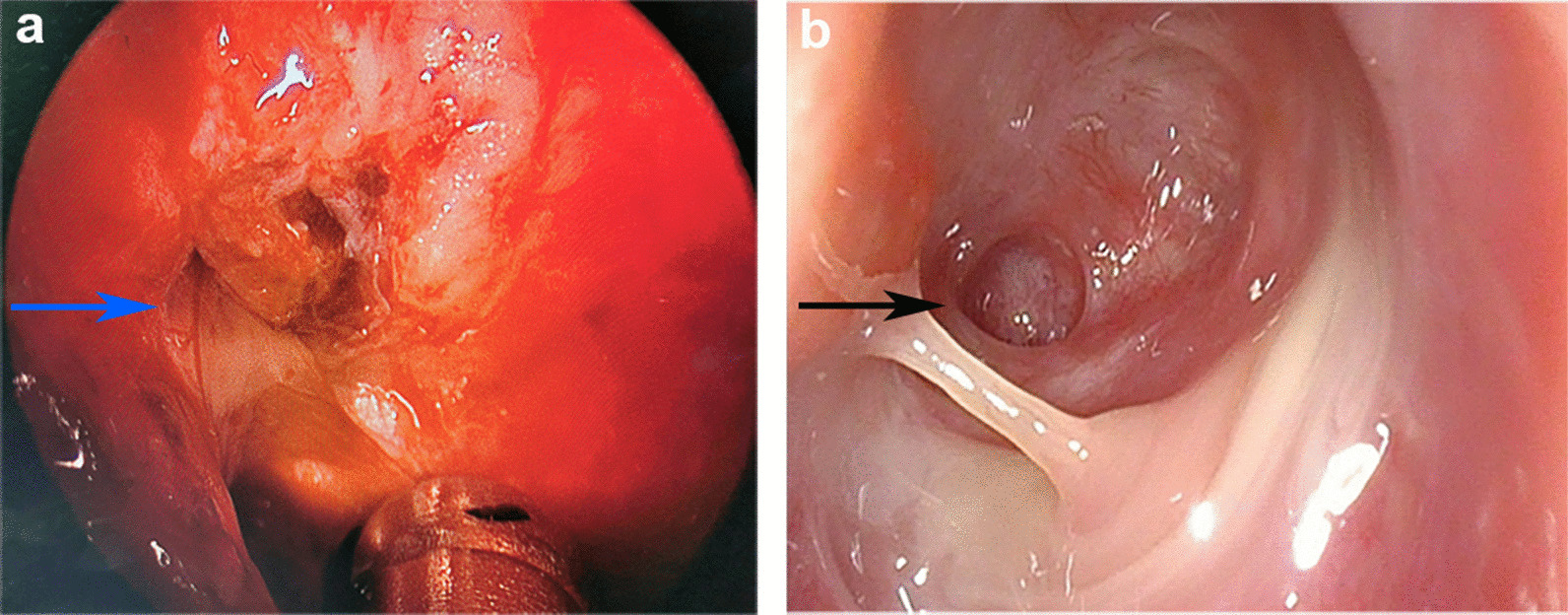
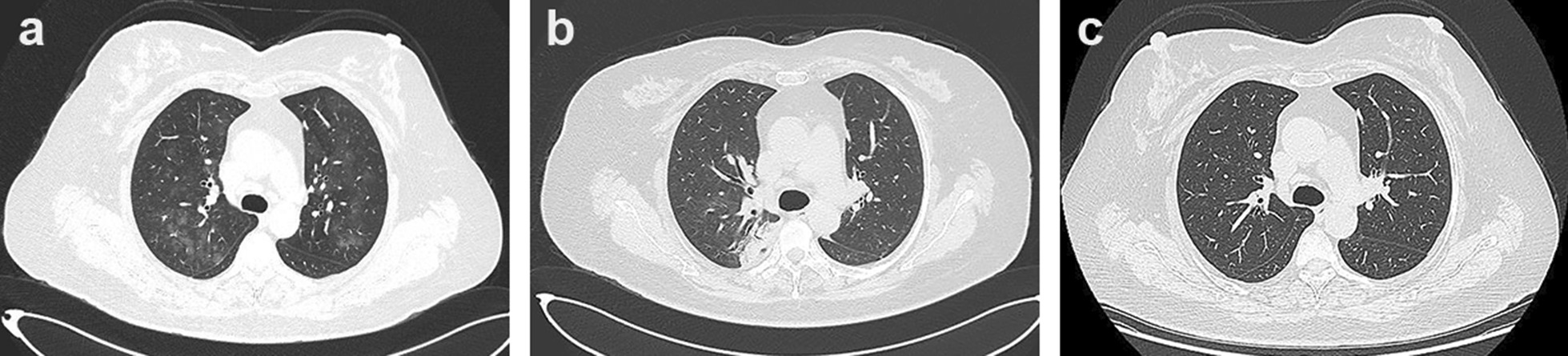
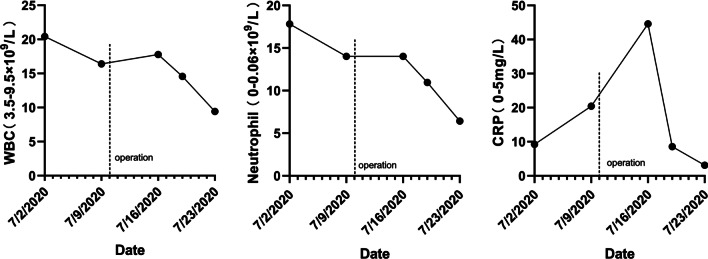
Case presentation: We present a case of a patient with 4 weeks of right-sided watery rhinorrhea accompanied by intermittent postnasal drip and dry cough as the main symptoms. Combined with clinical symptoms, imaging examination of the sinuses, and laboratory examination of nasal secretions, she was initially diagnosed as spontaneous sphenoid sinus meningoencephalocele with CSF rhinorrhea, and intraoperative endoscopic findings and postoperative pathology also confirmed this diagnosis. Her chest computed tomography showed multiple flocculent ground glass density shadows in both lungs on admission. The patient underwent endoscopic resection of meningoencephalocele and repair of skull base defect after she was ruled out of viral pneumonitis. Symptoms of rhinorrhea and dry cough disappeared, and pneumonitis was improved 1 week after surgery and cured 2 months after surgery. Persistent CSF rhinorrhea caused by spontaneous sphenoid sinus meningoencephalocele was eventually found to be a major etiology for aspiration pneumonitis although the absence of typical symptoms and well-defined risk factors for aspiration, such as dysphagia, impaired cough reflex and reflux diseases.
Conclusions: We report a rare case of aspiration pneumonitis caused by spontaneous sphenoid sinus meningoencephalocele with CSF rhinorrhea, which can bring more attention and understanding to the uncommon etiology for aspiration, so as to make more accurate diagnosis of the disease and early surgical treatment.
Keywords: Aspiration pneumonitis; Etiology; Meningoencephalocele; Postnasal drip; Sphenoid sinus.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Analysis of the Causes and Experience in the Diagnosis and Treatment of Meningocele Caused by Sternberg's Canal of the Sphenoid Sinus: Two Case Reports and a Review of the Literature.Curr Med Imaging. 2023;19(9):1063-1070. doi: 10.2174/1573405619666230206103036. Curr Med Imaging. 2023. PMID: 36748216 Review.
-
Chronic Aspiration Pneumonitis Caused by Spontaneous Cerebrospinal Fluid Fistulae of the Skull Base.Laryngoscope. 2021 Mar;131(3):462-466. doi: 10.1002/lary.28757. Epub 2020 May 25. Laryngoscope. 2021. PMID: 32449957
-
A case of sphenoid sinus meningoencephalocele repaired by an image-guided endoscopic endonasal approach.Auris Nasus Larynx. 2011 Oct;38(5):632-7. doi: 10.1016/j.anl.2011.01.015. Epub 2011 Mar 9. Auris Nasus Larynx. 2011. PMID: 21392906
-
Transcranial approach for spontaneous CSF rhinorrhea due to Sternberg's canal intrasphenoidal meningoencephalocele: case report and review of the literature.Turk Neurosurg. 2012;22(2):242-5. doi: 10.5137/1019-5149.JTN.2902-10.1. Turk Neurosurg. 2012. PMID: 22437302 Review.
-
Endoscopic management of spontaneous meningoencephalocele of the lateral sphenoid sinus.J Neurosurg. 2010 May;112(5):1070-7. doi: 10.3171/2009.7.JNS0842. J Neurosurg. 2010. PMID: 19698044
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
