

Enhanced interfragmentary stability and improved clinical prognosis with use of the off-axis screw technique to treat vertical femoral neck fractures in nongeriatric patients
- PMID: 34332590
- PMCID: PMC8325251
- DOI: 10.1186/s13018-021-02619-8
Enhanced interfragmentary stability and improved clinical prognosis with use of the off-axis screw technique to treat vertical femoral neck fractures in nongeriatric patients
Abstract
Background: The optimal internal fixation strategy for vertical femoral neck fractures (VFNFs) in nongeriatric patients remains uncertain. Therefore, the purpose of this study was to compare the clinical prognoses and underlying mechanical characteristics of a novel off-axis screw technique with dynamic hip screws (DHSs) and three traditional parallel screws.
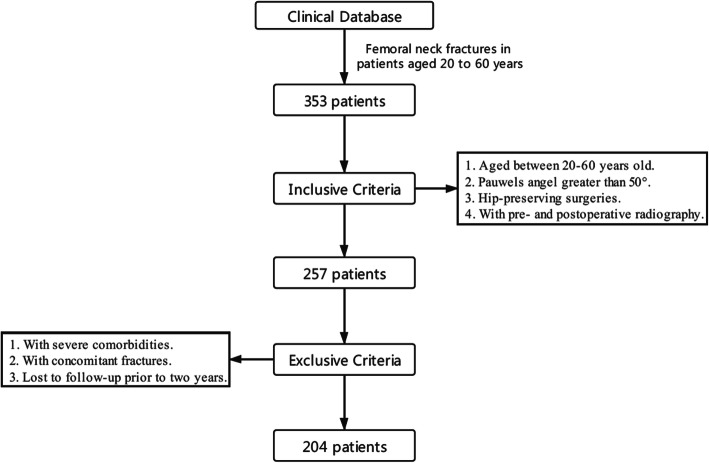
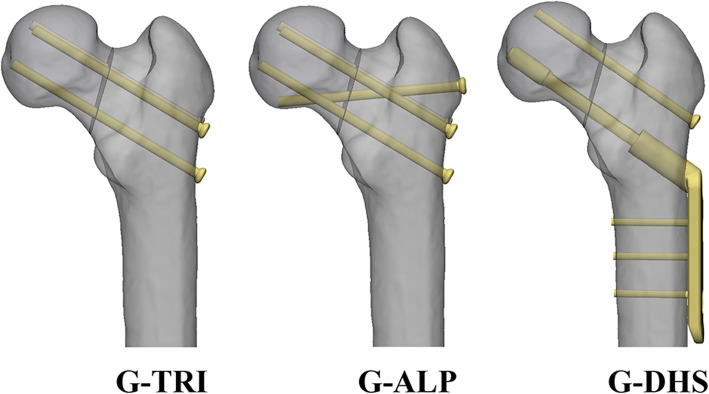
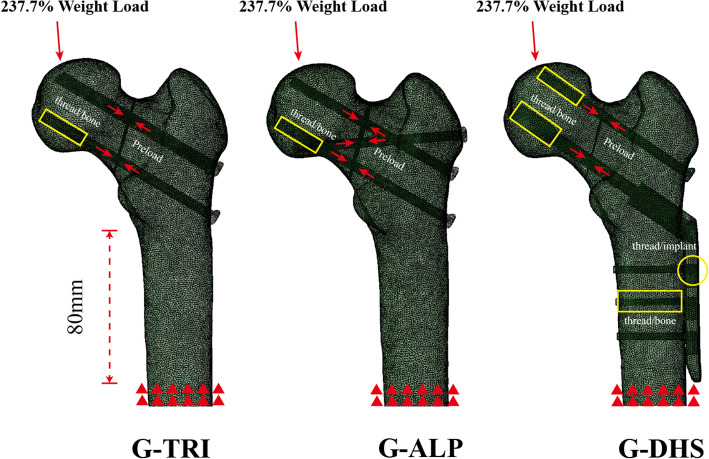
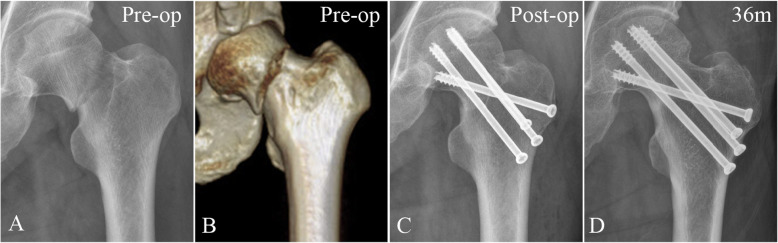
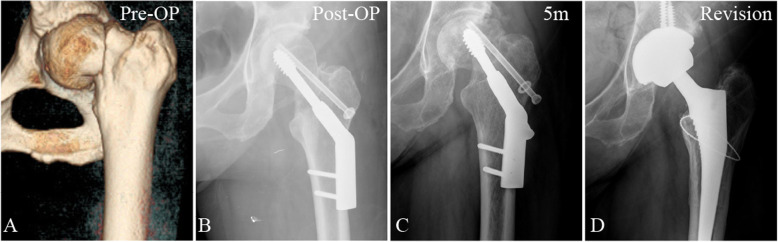
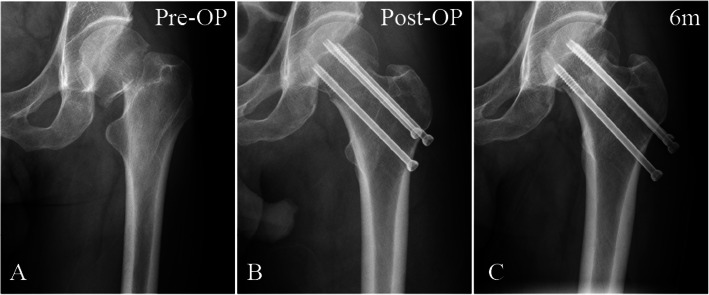
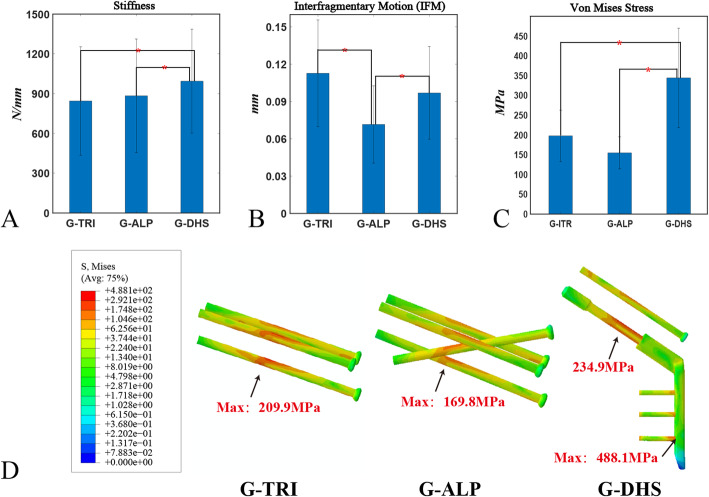
Methods: This study included a clinical investigation and a patient-specific finite element analysis (FEA). In the clinical investigation, VFNF patients were grouped by fixation type: (1) use of three parallel screws (G-TRI); (2) augmentation with an off-axis screw (G-ALP); and (3) DHS with an anti-rotational screw (G-DHS). Fixation failures (nonunion, femoral neck shortening (FNS), varus deformation, screw cut-out) and avascular necrosis (AVN) consequent to the three types of fixations were compared. In the FEA, twenty-four fixation models with the three fixation types were created based on the data of eight healthy volunteers. Models were assessed under walking conditions. Stiffness, interfragmentary motion (IFM), and implant stress were evaluated.
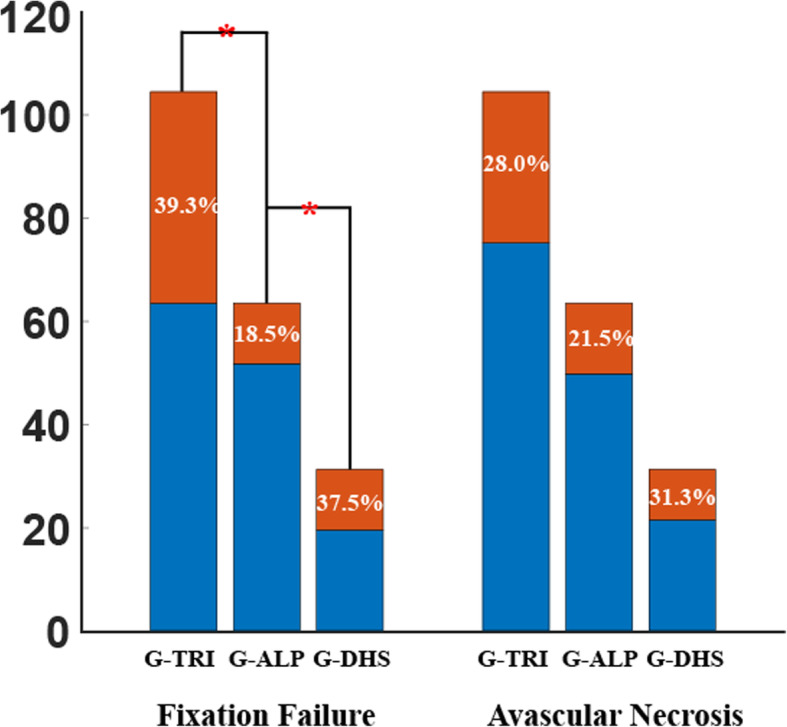
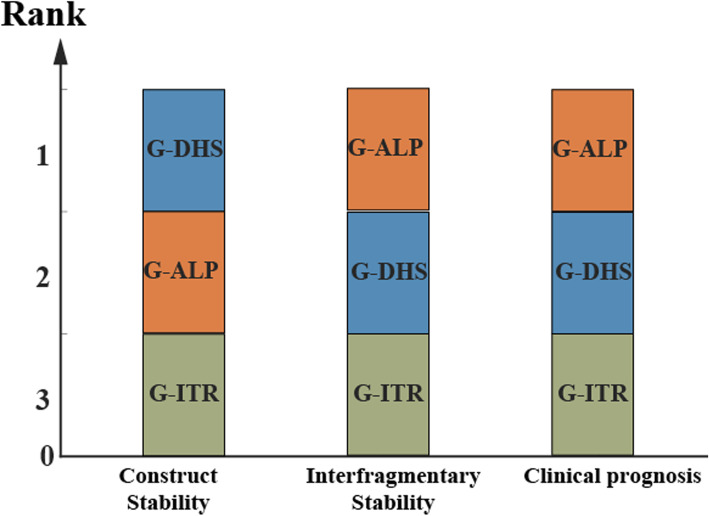
Results: In the clinical investigation, the fixation failure rate was significantly (p < 0.05) lower in G-ALP (18.5%) than in G-DHS (37.5%) and G-TRI (39.3%). No significant difference in AVN was observed among the three fixation groups. In the FEA, stiffness and implant stress in the G-DHS models were significantly (p < 0.05) higher, and the IFM of G-ALP was significantly (p < 0.05) lower among the groups.
Conclusions: Among fixation types for VFNFs, the off-axis screw technique exhibited better interfragmentary stability (lowest IFM) and a lower fixation failure rate (especially FNS). Analyzing interfragmentary stability in biomechanical experiments is more consistent with clinical prognosis than construct stability for VFNFs, suggesting that internal fixations should aim for this outcome.
Keywords: Biomechanical study; Clinical study; Cross-screw technique; Internal fixation; Vertical femoral neck fractures.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
What makes vertical femoral neck fracture with posterior inferior comminution different? An analysis of biomechanical features and optimal internal fixation strategy.Injury. 2023 Aug;54(8):110842. doi: 10.1016/j.injury.2023.110842. Epub 2023 May 29. Injury. 2023. PMID: 37296009
-
Long-term differences in clinical prognosis between crossed- and parallel-cannulated screw fixation in vertical femoral neck fractures of non-geriatric patients.Injury. 2021 Nov;52(11):3408-3414. doi: 10.1016/j.injury.2021.07.014. Epub 2021 Jul 10. Injury. 2021. PMID: 34281695
-
Biomechanical evaluation of different internal fixation methods based on finite element analysis for Pauwels type III femoral neck fracture.Injury. 2022 Oct;53(10):3115-3123. doi: 10.1016/j.injury.2022.08.038. Epub 2022 Aug 18. Injury. 2022. PMID: 35999063
-
Comparison of young femoral neck fractures treated by femoral neck system, multiple cancellous screws and dynamic hip screws: a retrospectively comparison study.BMC Musculoskelet Disord. 2024 Mar 2;25(1):188. doi: 10.1186/s12891-024-07319-y. BMC Musculoskelet Disord. 2024. PMID: 38431562 Free PMC article. Review.
-
Biomechanical Evaluation of Internal Fixation of Pauwels Type III Femoral Neck Fractures: A Systematic Review of Various Fixation Methods.Clin Orthop Surg. 2019 Mar;11(1):1-14. doi: 10.4055/cios.2019.11.1.1. Epub 2019 Feb 18. Clin Orthop Surg. 2019. PMID: 30838102 Free PMC article.
Cited by
-
The Effect of Vertical and Oblique Inclinations on Fracture Stability and Reoperation Risks in Femoral-Neck Fractures of Nongeriatric Patient.Front Bioeng Biotechnol. 2021 Nov 3;9:782001. doi: 10.3389/fbioe.2021.782001. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34805128 Free PMC article.
-
[Effectiveness of guide plate with mortise-tenon joint structure combined with off-axis fixation in treatment of Pauwels type Ⅲ femoral neck fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025 Mar 15;39(3):284-289. doi: 10.7507/1002-1892.202411083. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025. PMID: 40101902 Free PMC article. Chinese.
-
Computational modeling of bone allograft reconstruction following femoral shaft tumor resection: Investigating the impact of supplementary plate fixation.PLoS One. 2025 Feb 6;20(2):e0316719. doi: 10.1371/journal.pone.0316719. eCollection 2025. PLoS One. 2025. PMID: 39913461 Free PMC article.
-
Nine-year-long complex humeral nonunion salvaged by distraction osteogenesis technique: a case report and review of the literature.BMC Surg. 2022 Mar 3;22(1):77. doi: 10.1186/s12893-022-01524-z. BMC Surg. 2022. PMID: 35241038 Free PMC article. Review.
-
Biomechanical properties of off-axis screw in the treatment of vertical femoral neck fractures: a finite element analysis.BMC Musculoskelet Disord. 2025 May 15;26(1):479. doi: 10.1186/s12891-025-08722-9. BMC Musculoskelet Disord. 2025. PMID: 40375182 Free PMC article.
References
-
- Luttrell K, Beltran M, Collinge CA. Preoperative decision making in the treatment of high-angle “vertical” femoral neck fractures in young adult patients. An expert opinion survey of the Orthopaedic Trauma Association's (OTA) membership. J Orthop Trauma. 2014;28(9):e221–e225. doi: 10.1097/bot.0000000000000080. - DOI - PubMed
-
- Management of acute hip fracture. N Engl J Med. 2018;378(10):971–2. 10.1056/NEJMc1800044. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
