

Incorporation of an intercostal catheter into a multimodal analgesic strategy for uniportal video-assisted thoracoscopic surgery: a feasibility study
- PMID: 34332605
- PMCID: PMC8325303
- DOI: 10.1186/s13019-021-01590-z
Incorporation of an intercostal catheter into a multimodal analgesic strategy for uniportal video-assisted thoracoscopic surgery: a feasibility study
Abstract
Background: Well-controlled postoperative pain is essential for early recovery after uniportal video-assisted thoracoscopic surgery (UVATS). Conventional analgesia like opioids and thoracic epidural anaesthesia have been associated with hypotension and urinary retention. Intercostal catheters are a regional analgesic alternative that can be inserted during UVATS to avoid these adverse effects. This feasibility study aims to evaluate the postoperative pain scores and analgesic requirements with incorporation of an intercostal catheter into a multimodal analgesic strategy for UVATS.
Methods: In this observational study, 26 consecutive patients who underwent UVATS were administered a multilevel intercostal block and oral paracetamol. All of these patients received 0.2% ropivacaine continuously at 4 ml/h via an intercostal catheter at the level of the incision. Rescue analgesia including etoricoxib, gabapentin and opioids were prescribed using a pain ladder approach. Postoperative pain scores and analgesic usage were assessed. The secondary outcomes were postoperative complications, days to ambulation and length of stay.
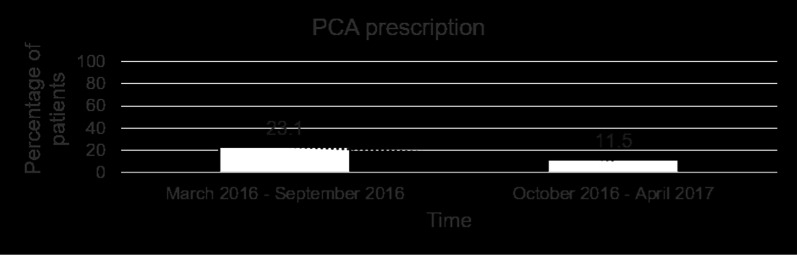
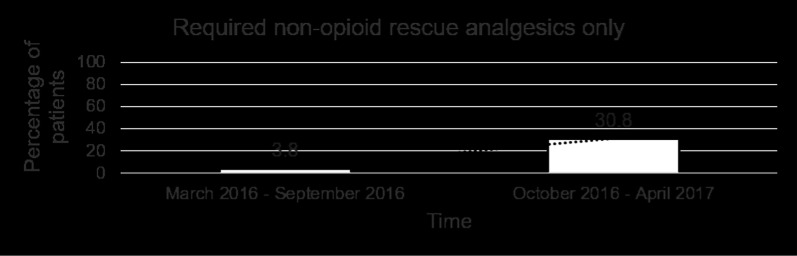
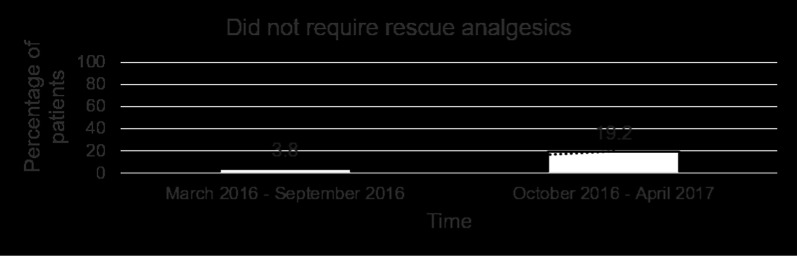
Results: No technical difficulties were encountered during placement of the intercostal catheter. There was only one case of peri-catheter leakage. Mean pain score was 0.31 (range 0-2) on post-operative day 1 and was 0.00 by post-operative day 5. 16 patients (61.6%) required only oral rescue analgesia. The number of patients who required rescue non-opioids only increased from 1 in the first 7 months to 8 in the next 7 months. There were no cases of hypotension or urinary retention. Median time to ambulation was 1 day (range 1-2). Mean post-operative length of stay was 4.17 ± 2.50 days.
Conclusions: Incorporation of an intercostal catheter into a multimodal analgesia strategy for UVATS is feasible and may provide adequate pain control with decreased opioid usage.
Keywords: Intercostal catheter; ON-Q pain relief system; Postoperative recovery after thoracic surgery; Subpleural analgesia; Uniportal video-assisted thoracoscopic surgery (UVATS).
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of the analgesic effect of ultrasound-guided paravertebral block and ultrasound-guided retrolaminar block in Uniportal video-assisted Thoracoscopic surgery: a prospective, randomized study.BMC Cancer. 2021 Nov 16;21(1):1229. doi: 10.1186/s12885-021-08938-7. BMC Cancer. 2021. PMID: 34784889 Free PMC article. Clinical Trial.
-
Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracic surgery: a study protocol for a prospective randomized open label non-inferiority trial.Trials. 2021 May 4;22(1):321. doi: 10.1186/s13063-021-05275-9. Trials. 2021. PMID: 33947442 Free PMC article.
-
Risk and benefit analysis of single-shot nerve block for postoperative analgesia for uniportal video-assisted thoracic surgery (uVATS): a randomized controlled trial.BMC Anesthesiol. 2025 Feb 12;25(1):68. doi: 10.1186/s12871-025-02955-w. BMC Anesthesiol. 2025. PMID: 39939956 Free PMC article. Clinical Trial.
-
Developments in Postoperative Analgesia in Open and Minimally Invasive Thoracic Surgery Over the Past Decade.Semin Thorac Cardiovasc Surg. 2024 Autumn;36(3):378-385. doi: 10.1053/j.semtcvs.2023.07.002. Epub 2023 Sep 30. Semin Thorac Cardiovasc Surg. 2024. PMID: 37783320 Review.
-
Postthoracotomy pain management.Chest Surg Clin N Am. 2002 May;12(2):251-63. doi: 10.1016/s1052-3359(02)00011-x. Chest Surg Clin N Am. 2002. PMID: 12122825 Review.
Cited by
-
The effect of continuous intercostal nerve block vs. single shot on analgesic outcomes and hospital stays in minimally invasive direct coronary artery bypass surgery: a retrospective cohort study.BMC Anesthesiol. 2022 Mar 8;22(1):64. doi: 10.1186/s12871-022-01607-7. BMC Anesthesiol. 2022. PMID: 35260084 Free PMC article.
-
The impact of hydromorphone combined with ropivacaine in serratus anterior plane block on postoperative pain in patients undergoing video-assisted thoracoscopic pulmonary lobectomy: a randomized, double-blind clinical trial.BMC Anesthesiol. 2025 May 10;25(1):237. doi: 10.1186/s12871-025-03101-2. BMC Anesthesiol. 2025. PMID: 40348971 Free PMC article. Clinical Trial.
-
A balancing act-the role of opioid-sparing anesthesia in enhancing recovery after thoracic surgery.J Thorac Dis. 2022 Sep;14(9):3122-3124. doi: 10.21037/jtd-22-1086. J Thorac Dis. 2022. PMID: 36245573 Free PMC article. No abstract available.
-
Protocol for a randomised controlled trial: optimisation of perioperative analgesia protocol for uniportal video-assisted thoracoscopic surgery.BMJ Open. 2024 Apr 2;14(4):e079434. doi: 10.1136/bmjopen-2023-079434. BMJ Open. 2024. PMID: 38569709 Free PMC article.
-
Opioid prescription guideline is important to enhanced recovery after thoracic surgery protocol.J Thorac Dis. 2023 Oct 31;15(10):5275-5277. doi: 10.21037/jtd-23-1208. Epub 2023 Sep 6. J Thorac Dis. 2023. PMID: 37969260 Free PMC article. No abstract available.
References
-
- Elmore B, Nguyen V, Blank R, Yount Y, Lau C. Pain management following thoracic surgery. Thorac Surg Clin. 2015;25:393–409. - PubMed
-
- Yeap YL, Wolfe JW, Backfish-White KM, Young JV, Stewart J, Ceppa DP, et al. Randomized prospective study evaluating single-injection paravertebral block, paravertebral catheter, and thoracic epidural catheter for postoperative regional analgesia after video-assisted thoracoscopic surgery. J Cardiothorac Vasc Anesth. 2020;34:1870–1876. - PubMed
-
- Kosinski S, Fryzlewicz E, Wilkojc M, Cmiel A, Zielinski M. Comparison of continuous epidural block and continuous paravertebral block in postoperative analgesia after video-assisted thoracoscopic surgery lobectomy: a randomised, non-inferiority trial. Anaesthesiol Intensive Ther. 2016;48:280–287. - PubMed
-
- Okajima H, Tanaka O, Ushio M, Higushi Y, Nagai Y, Iijima K, et al. Ultrasound-guided continuous thoracic paravertebral block provides comparable analgesia and fewer episodes of hypotension than continuous epidural block after lung surgery. J Anesth. 2015;29:373–378. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
