

Tannin-phytobezoars with Gastric Outlet Obstruction Treated by Dissolution with Administration and Endoscopic Injection of Coca-Cola®, Endoscopic Crushing, and Removal (with Video)
- PMID: 34334573
- PMCID: PMC8866791
- DOI: 10.2169/internalmedicine.8090-21
Tannin-phytobezoars with Gastric Outlet Obstruction Treated by Dissolution with Administration and Endoscopic Injection of Coca-Cola®, Endoscopic Crushing, and Removal (with Video)
Abstract
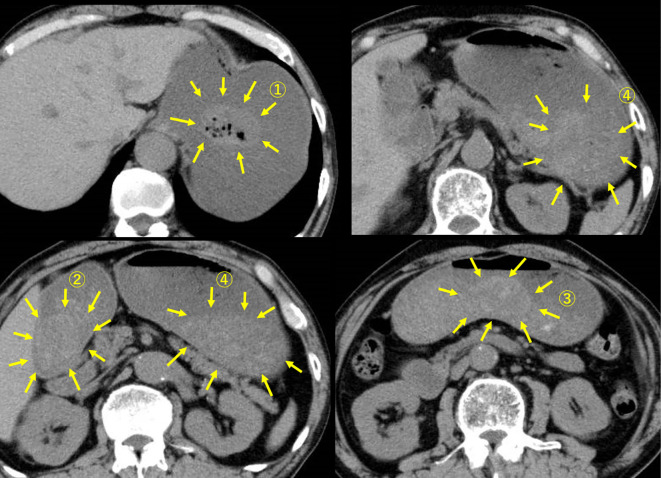
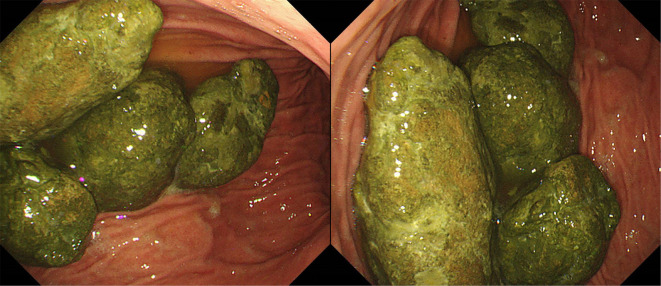
A 77-year-old man complained of postmeal vomiting and sustained general fatigue. An abdominal computed tomography scan showed massive gastric expansion and fluid storage. Gastroscopy revealed four gastric bezoars that were considered to have caused pyloric ring obstruction. The patient was asked to drink 500 mL per day of Coca-Cola® for 4 days. On the fourth day, we performed endoscopic crushing and removal by injecting Coca-Cola®, cutting the softened bezoar with endoscopic snares, and collecting the pieces with endoscopic nets. We herein report (with a video presentation) a rare case of tannin-phytobezoars endoscopically removed with the administration and injection of Coca-Cola®.
Keywords: Coca-Cola®; endoscopic surgery; gastric bezoars; gastric outlet obstruction; phytobezoars; tannin.
Conflict of interest statement
Figures

Similar articles
-
Successful treatment with a combination of endoscopic injection and irrigation with coca cola for gastric bezoar-induced gastric outlet obstruction.J Chin Med Assoc. 2008 Jan;71(1):49-52. doi: 10.1016/S1726-4901(08)70073-X. J Chin Med Assoc. 2008. PMID: 18218561
-
Gastric Outlet Obstruction--An Unexpected Complication during Coca-Cola Therapy for a Gastric Bezoar: A Case Report and Literature Review.Intern Med. 2016;55(9):1085-9. doi: 10.2169/internalmedicine.55.5567. Epub 2016 May 1. Intern Med. 2016. PMID: 27150859 Review.
-
Systematic review: Coca-Cola can effectively dissolve gastric phytobezoars as a first-line treatment.Aliment Pharmacol Ther. 2013 Jan;37(2):169-73. doi: 10.1111/apt.12141. Aliment Pharmacol Ther. 2013. PMID: 23252775
-
Huge gastric diospyrobezoars successfully treated by oral intake and endoscopic injection of Coca-Cola.Dig Liver Dis. 2006 Jul;38(7):515-7. doi: 10.1016/j.dld.2005.10.024. Epub 2005 Dec 5. Dig Liver Dis. 2006. PMID: 16330268
-
Gastric Bezoar Treatment by Endoscopic Fragmentation in Combination with Pepsi-Cola® Administration.Am J Case Rep. 2015 Jul 10;16:445-8. doi: 10.12659/AJCR.893786. Am J Case Rep. 2015. PMID: 26164451 Free PMC article.
Cited by
-
Effect of Coca-Cola on the Dissolution of Persimmon-Related Phytobezoar in a Tertiary Care Hospital.Cureus. 2024 Feb 18;16(2):e54420. doi: 10.7759/cureus.54420. eCollection 2024 Feb. Cureus. 2024. PMID: 38510864 Free PMC article.
-
Self-disassembling nanoparticles as oral nanotherapeutics targeting intestinal microenvironment.Nat Commun. 2025 Apr 9;16(1):3365. doi: 10.1038/s41467-025-58513-y. Nat Commun. 2025. PMID: 40204740 Free PMC article.
-
Severe Airway Obstruction Caused by Esophageal Bezoar with Coca-Cola and Creon (Pancrelipase) in a Patient with Underlying Achalasia: A Comprehensive Case Report.Case Rep Gastrointest Med. 2024 Jul 27;2024:2081040. doi: 10.1155/2024/2081040. eCollection 2024. Case Rep Gastrointest Med. 2024. PMID: 39104748 Free PMC article.
-
Trichobezoar effectively treated with direct endoscopic injection of Coca-Cola: A case report.DEN Open. 2023 Sep 25;4(1):e283. doi: 10.1002/deo2.283. eCollection 2024 Apr. DEN Open. 2023. PMID: 37753229 Free PMC article.
-
Treatment of giant fecalith colonic obstruction in a patient with Duchenne muscular dystrophy using endoscopic injection of hydrogen peroxide: a case report and literature review.Front Med (Lausanne). 2024 Dec 4;11:1456246. doi: 10.3389/fmed.2024.1456246. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39703526 Free PMC article.