

Acromegaly Cases Exhibiting Increased Growth Hormone Levels during Oral Glucose Loading with Preadministration of Dipeptidyl Peptidase-4 Inhibitor
- PMID: 34334589
- PMCID: PMC8381171
- DOI: 10.2169/internalmedicine.4755-20
Acromegaly Cases Exhibiting Increased Growth Hormone Levels during Oral Glucose Loading with Preadministration of Dipeptidyl Peptidase-4 Inhibitor
Abstract
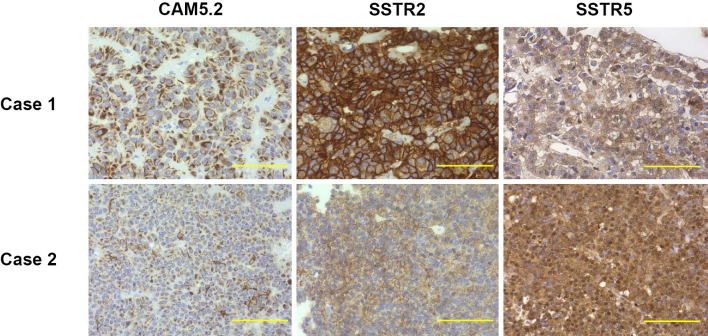
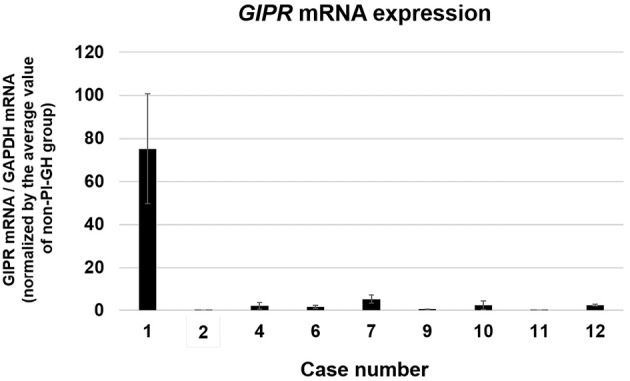
Objective Glucose-dependent insulinotropic polypeptide (GIP) is speculated to worsen growth hormone (GH) hypersecretion in acromegaly and to be a cause of paradoxical increases in GH (PI-GH) during 75-g oral glucose tolerance testing (75-g OGTT). Dipeptidyl peptidase-4 inhibitors (DPP4is), which increase the circulating concentration of active GIP, are frequently administered to diabetic patients, including those with acromegaly. We aimed to determine whether or not the administration of a DPP4i increases GH concentration, especially in patients demonstrating PI-GH during a DPP4i-OGTT, in which a DPP4i was administered immediately before 75-g OGTT. Methods This prospective cross-sectional study was carried out on acromegalic patients admitted to Hokkaido University hospital between June 2011 and May 2018. The participants underwent both 75-g OGTT and DPP4i-OGTT. For those who underwent surgery, immunohistochemical staining and quantitative polymerase chain reaction (PCR) for the GIP receptor (GIPR) were performed on the resected pituitary adenomas. Results Twenty-five percent of the participants had PI-GH confirmed (3 of 12 cases). Two of the three participants who demonstrated PI-GH exhibited higher circulating GH concentrations during DPP4i-OGTT than during OGTT. The increase in plasma glucose was reduced during DPP4i-OGTT compared to during 75-g OGTT, suggesting that the increase in GH during DPP4i-OGTT was due not to high glucose concentrations but instead increased GIP caused by the administration of DPP4i. The adenoma from one participant with PI-GH displayed positive immunostaining for GIPR and a higher GIPR messenger ribonucleic acid (mRNA) expression than the others. Conclusion DPP4i may enhance the GH secretion response during glucose loading, especially in individuals with PI-GH.
Keywords: acromegaly; glucose-dependent insulinotropic polypeptide; growth hormone.
Conflict of interest statement
Hideaki Miyoshi: Honoraria, Astellas Pharma, AstraZeneca, Dainippon Pharma, Eli Lilly, Mitsubishi Tanabe Pharma, MSD, Boehringer Ingelheim, Novo Nordisk Pharma, Kowa Pharmaceutical, Ono Pharmaceutical and Sanofi; Research funding, Astellas Pharma, AstraZeneca, Daiichi Sankyo, Dainippon Pharma, Eli Lilly, Mitsubishi Tanabe Pharma, MSD, Novo Nordisk Pharma, Kowa Pharmaceutical, Ono Pharmaceutical, Boehringer Ingelheim, Johnson & Johnson, Abbott Japan and Taisho Toyama Pharmaceutical. Yukihiro Fujita: Honoraria, MSD, Novo Nordisk, Sanofi, Taisho-Toyama, Takeda Pharmaceutical, Dainippon-Sumitomo, Astellas Pharma and Ono Pharmaceutical. Akinobu Nakamura: Research funding, AstraZeneca, LifeScan Japan and Taisho Pharmaceutical. So Nagai: Honoraria, Eli Lilly. Tatsuya Atsumi: Honoraria, Mitsubishi Tanabe Pharma, Chugai Pharmaceutical, Astellas Pharma, Takeda Pharmaceutical, Pfizer, AbbVie, Eisai, Daiichi Sankyo, Bristol-Myers Squibb, UCB Japan and Eli Lilly Japan; Research funding, Astellas Pharma, Takeda Pharmaceutical, Mitsubishi Tanabe Pharma, Chugai Pharmaceutical, Daiichi Sankyo, Otsuka Pharmaceutical, Pfizer and Alexion.
Figures


References
-
- Arafat AM, Möhlig M, Weickert MO, et al. Growth hormone response during oral glucose tolerance test: the impact of assay method on the estimation of reference values in patients with acromegaly and in healthy controls, and the role of gender, age, and body mass index. J Clin Endocrinol Metab 93: 1254-1262, 2008. - PubMed
-
- Hage M, Kamenický P, Chanson P. Growth hormone response to oral glucose load: from normal to pathological conditions. Neuroendocrinology 108: 244-255, 2019. - PubMed
-
- Melmed S. Acromegaly. N Engl J Med 322: 966-977, 1990. - PubMed
-
- Umahara M, Okada S, Ohshima K, Mori M. Glucose-dependent insulinotropic polypeptide induced growth hormone secretion in acromegaly. Endocr J 50: 643-650, 2003. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous