

Diagnosing small fiber neuropathy in clinical practice: a deep phenotyping study
- PMID: 34335876
- PMCID: PMC8283814
- DOI: 10.1177/17562864211004318
Diagnosing small fiber neuropathy in clinical practice: a deep phenotyping study
Erratum in
-
Corrigendum to "Diagnosing small fiber neuropathy in clinical practice: a deep phenotyping study".Ther Adv Neurol Disord. 2021 Jul 31;14:17562864211036650. doi: 10.1177/17562864211036650. eCollection 2021. Ther Adv Neurol Disord. 2021. PMID: 34377152 Free PMC article.
Abstract
Background and aims: Small fiber neuropathy (SFN) is increasingly suspected in patients with pain of uncertain origin, and making the diagnosis remains a challenge lacking a diagnostic gold standard.
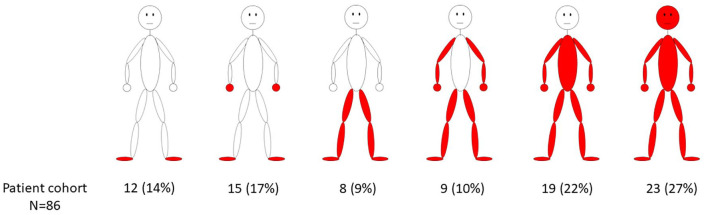
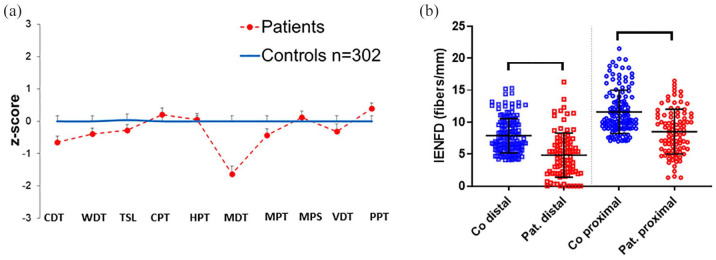
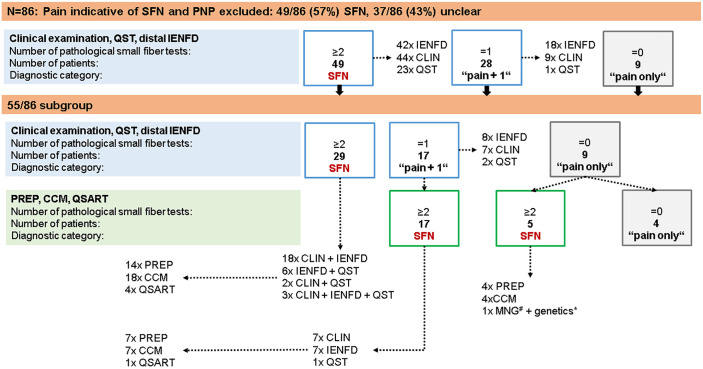
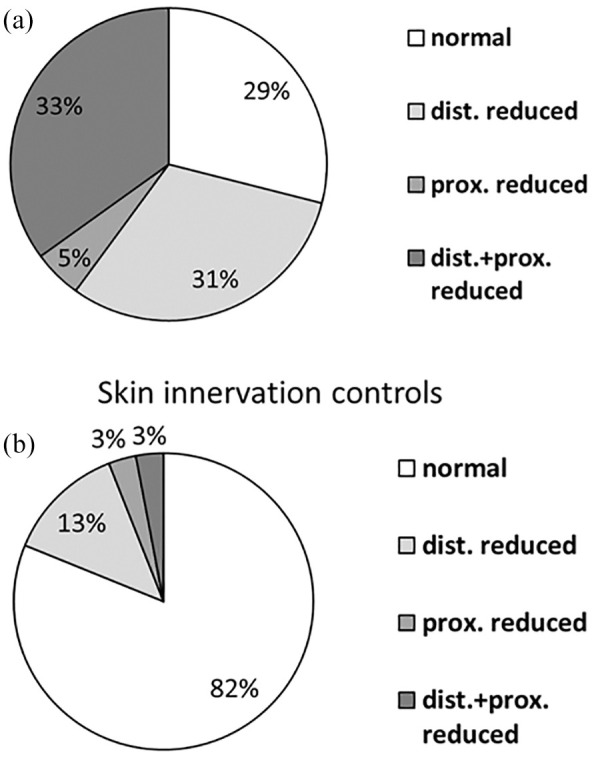
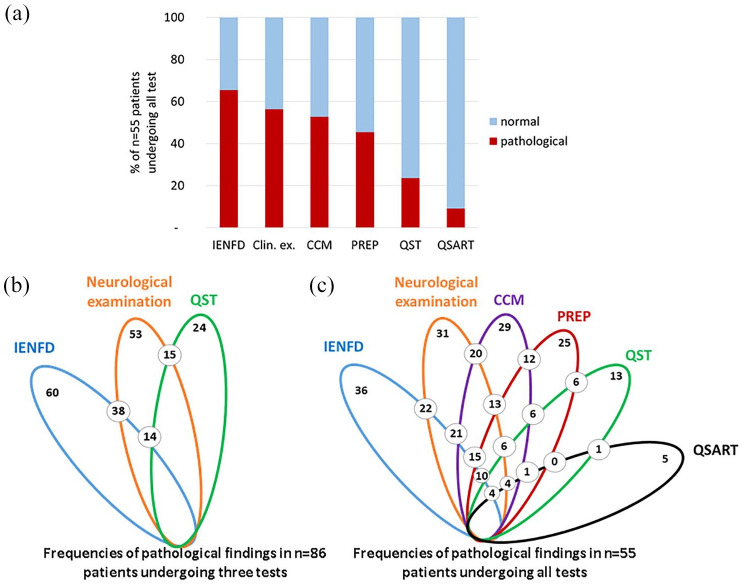
Methods: In this case-control study, we prospectively recruited 86 patients with a medical history and clinical phenotype suggestive of SFN. Patients underwent neurological examination, quantitative sensory testing (QST), and distal and proximal skin punch biopsy, and were tested for pain-associated gene loci. Fifty-five of these patients additionally underwent pain-related evoked potentials (PREP), corneal confocal microscopy (CCM), and a quantitative sudomotor axon reflex test (QSART).
Results: Abnormal distal intraepidermal nerve fiber density (IENFD) (60/86, 70%) and neurological examination (53/86, 62%) most frequently reflected small fiber disease. Adding CCM and/or PREP further increased the number of patients with small fiber impairment to 47/55 (85%). Genetic testing revealed potentially pathogenic gene variants in 14/86 (16%) index patients. QST, QSART, and proximal IENFD were of lower impact.
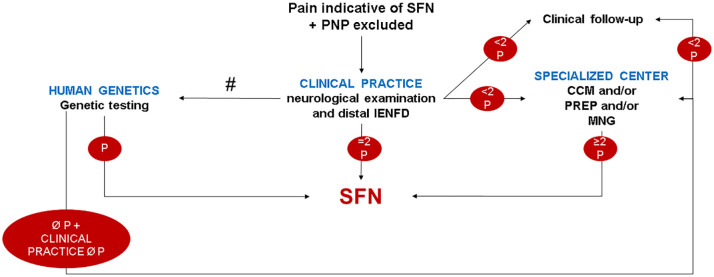
Conclusion: We propose to diagnose SFN primarily based on the results of neurological examination and distal IENFD, with more detailed phenotyping in specialized centers.
Keywords: algorithm; diagnosis; neurological examination; skin punch biopsy; small fiber neuropathy.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: N.S., C.M.z.A., L.K., F.G., K.E., B.N., T.M., A.K., D.K., I.K. report no conflicts of interest. C.S., R.A.M., N.Ü. have taken part in clinical studies associated with small fiber neuropathy (Biogen, Vertex).
Figures
References
-
- Terkelsen AJ, Karlsson P, Lauria G, et al. The diagnostic challenge of small fibre neuropathy: clinical presentations, evaluations, and causes. Lancet Neurol 2017; 16: 934–944. - PubMed
-
- Lacomis D. Small-fiber neuropathy. Muscle Nerve 2002; 26: 173–188. - PubMed
-
- Stewart JD, Low PA, Fealey RD. Distal small fiber neuropathy: results of tests of sweating and autonomic cardiovascular reflexes. Muscle Nerve 1992; 15: 661–665. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
