

Low-dose total body irradiation facilitates antitumoral Th1 immune responses
- PMID: 34335959
- PMCID: PMC8315067
- DOI: 10.7150/thno.61459
Low-dose total body irradiation facilitates antitumoral Th1 immune responses
Abstract
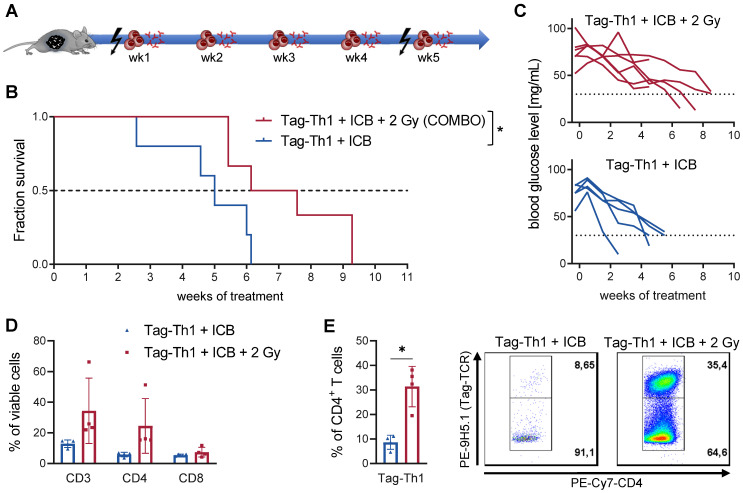
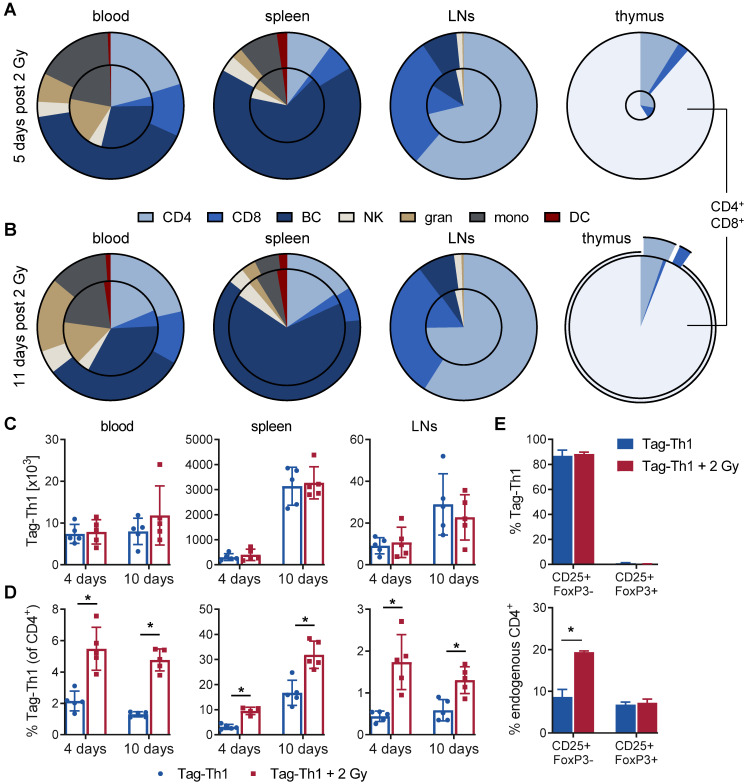
CD4+ T helper cells are capable of mediating long-term antitumoral immune responses. We developed a combined immunotherapy (COMBO) using tumor antigen-specific T helper 1 cells (Tag-Th1), dual PD-L1/LAG-3 immune checkpoint blockade, and a low-dose total body irradiation (TBI) of 2 Gy, that was highly efficient in controlling the tumor burden of non-immunogenic RIP1-Tag2 mice with late-stage endogenous pancreatic islet carcinomas. In this study, we aimed to explore the impact of 2 Gy TBI on the treatment efficacy and the underlying mechanisms to boost CD4+ T cell-based immunotherapies. Methods: Heavily progressed RIP1-Tag2 mice underwent COMBO treatment and their survival was compared to a cohort without 2 Gy TBI. Positron emission tomography/computed tomography (PET/CT) with radiolabeled anti-CD3 monoclonal antibodies and flow cytometry were applied to investigate 2 Gy TBI-induced alterations in the biodistribution of endogenous T cells of healthy C3H mice. Migration and homing properties of Cy5-labeled adoptive Tag-Th1 cells were monitored by optical imaging and flow cytometric analyses in C3H and tumor-bearing RIP1-Tag2 mice. Splenectomy or sham-surgery of late-stage RIP1-Tag2 mice was performed before onset of COMBO treatment to elucidate the impact of the spleen on the therapy response. Results: First, we determined a significant longer survival of RIP1-Tag2 mice and an increased CD4+ T cell tumor infiltrate when 2 Gy TBI was applied in addition to Tag-Th1 cell PD-L1/LAG-3 treatment. In non-tumor-bearing C3H mice, TBI induced a moderate host lymphodepletion and a tumor antigen-independent accumulation of Tag-Th1 cells in lymphoid and non-lymphoid organs. In RIP1-Tag2, we found increased numbers of effector memory-like Tag-Th1 and endogenous CD4+ T cells in the pancreatic tumor tissue after TBI, accompanied by a tumor-specific Th1-driven immune response. Furthermore, the spleen negatively regulated T cell effector function by upregulation PD-1/LAG-3/TIM-3 immune checkpoints, providing a further rationale for this combined treatment approach. Conclusion: Low-dose TBI represents a powerful tool to foster CD4+ T cell-based cancer immunotherapies by favoring Th1-driven antitumoral immunity. As TBI is a clinically approved and well-established technique it might be an ideal addition for adoptive cell therapy with CD4+ T cells in the clinical setting.
Keywords: RIP1-Tag2; T helper cells; Total body irradiation; cancer immunology; combined immunotherapy.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures




Similar articles
-
Cancer immunotherapy is accompanied by distinct metabolic patterns in primary and secondary lymphoid organs observed by non-invasive in vivo18F-FDG-PET.Theranostics. 2020 Jan 1;10(2):925-937. doi: 10.7150/thno.35989. eCollection 2020. Theranostics. 2020. PMID: 31903160 Free PMC article.
-
PD-L1-Independent Mechanisms Control the Resistance of Melanoma to CD4+ T Cell Adoptive Immunotherapy.J Immunol. 2018 May 1;200(9):3304-3311. doi: 10.4049/jimmunol.1701617. Epub 2018 Mar 30. J Immunol. 2018. PMID: 29602773
-
Irreversible electroporation combined with PD-L1/IL-6 dual blockade promotes anti-tumor immunity via cDC2/CD4+T cell axis in MHC-I deficient pancreatic cancer.Cancer Lett. 2025 May 1;617:217620. doi: 10.1016/j.canlet.2025.217620. Epub 2025 Mar 9. Cancer Lett. 2025. PMID: 40068706
-
Emerging immune checkpoints for cancer therapy.Acta Oncol. 2015 Nov;54(10):1706-13. doi: 10.3109/0284186X.2015.1071918. Epub 2015 Sep 11. Acta Oncol. 2015. PMID: 26361073 Review.
-
Overcoming the resistance of pancreatic cancer to immune checkpoint inhibitors.J Surg Oncol. 2017 Jul;116(1):55-62. doi: 10.1002/jso.24642. Epub 2017 Jun 19. J Surg Oncol. 2017. PMID: 28628715 Review.
Cited by
-
Pro- and Anti-Tumoral Factors Involved in Total Body Irradiation and Interleukin-2 Conditioning in Adoptive T Cell Therapy of Melanoma-Bearing Rag1 Knock-Out Mice.Cells. 2022 Dec 2;11(23):3894. doi: 10.3390/cells11233894. Cells. 2022. PMID: 36497152 Free PMC article.
-
In-depth cross-validation of human and mouse CD4-specific minibodies for noninvasive PET imaging of CD4+ cells and response prediction to cancer immunotherapy.Theranostics. 2024 Aug 1;14(12):4582-4597. doi: 10.7150/thno.95173. eCollection 2024. Theranostics. 2024. PMID: 39239511 Free PMC article.
-
Application of individualized multimodal radiotherapy combined with immunotherapy in metastatic tumors.Front Immunol. 2023 Jan 12;13:1106644. doi: 10.3389/fimmu.2022.1106644. eCollection 2022. Front Immunol. 2023. PMID: 36713375 Free PMC article. Review.
-
Effects of simulated space conditions on CD4+ T cells: a multi modal analysis.Front Immunol. 2024 Sep 2;15:1443936. doi: 10.3389/fimmu.2024.1443936. eCollection 2024. Front Immunol. 2024. PMID: 39286254 Free PMC article.
-
Evaluation of Short-Term Efficacy of PD-1 Monoclonal Antibody Immunotherapy for Lymphoma by Positron Emission Tomography/Computed Tomography Imaging with Convolutional Neural Network Image Registration Algorithm.Contrast Media Mol Imaging. 2022 Aug 31;2022:1388517. doi: 10.1155/2022/1388517. eCollection 2022. Contrast Media Mol Imaging. 2022. PMID: 36105450 Free PMC article.
References
-
- Doorduijn EM, Sluijter M, Salvatori DC, Silvestri S, Maas S, Arens R. et al. CD4(+) T Cell and NK Cell Interplay Key to Regression of MHC Class I(low) Tumors upon TLR7/8 Agonist Therapy. Cancer Immunol Res. 2017;5:642–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
