

Facial Nerve Monitoring under Different Levels of Neuromuscular Blockade with Cisatracurium Besilate in Parotid Tumour Surgery
- PMID: 34337032
- PMCID: PMC8298146
- DOI: 10.1155/2021/5655061
Facial Nerve Monitoring under Different Levels of Neuromuscular Blockade with Cisatracurium Besilate in Parotid Tumour Surgery
Retraction in
-
Retracted: Facial Nerve Monitoring under Different Levels of Neuromuscular Blockade with Cisatracurium Besilate in Parotid Tumour Surgery.Biomed Res Int. 2024 Mar 20;2024:9819172. doi: 10.1155/2024/9819172. eCollection 2024. Biomed Res Int. 2024. PMID: 38550067 Free PMC article.
Abstract
Background: Anaesthesia can alter neuronal excitability and vascular reactivity and ultimately lead to neurovascular coupling. Precise control of the skeletal muscle relaxant doses is the key in reducing anaesthetic damage.
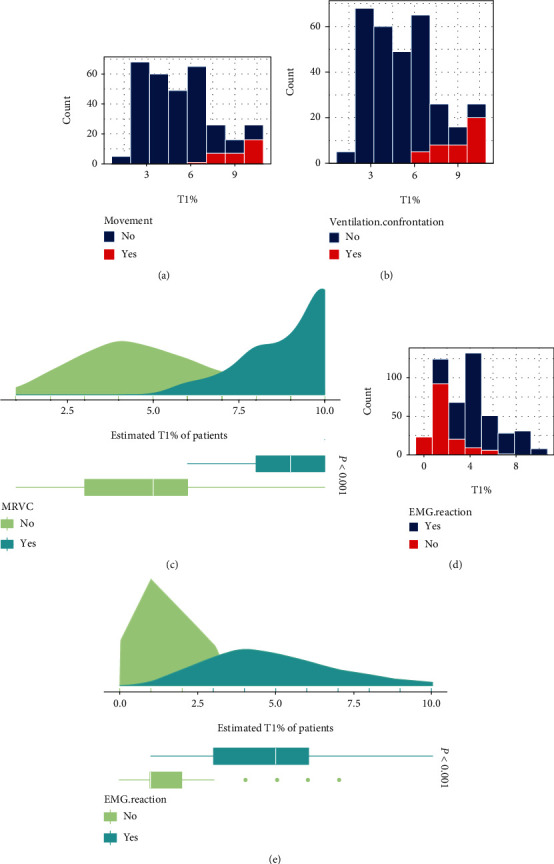
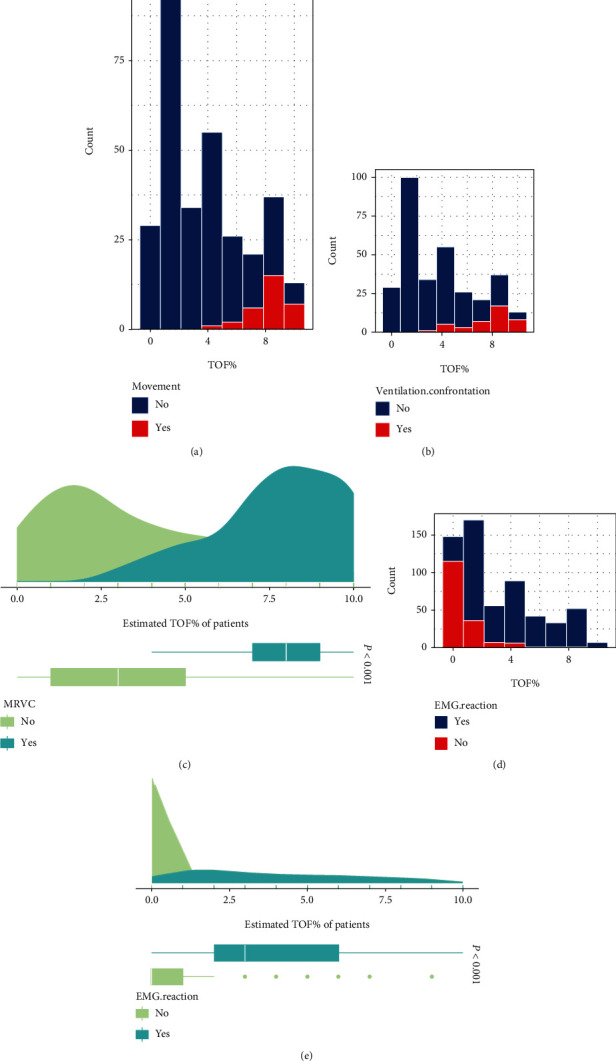
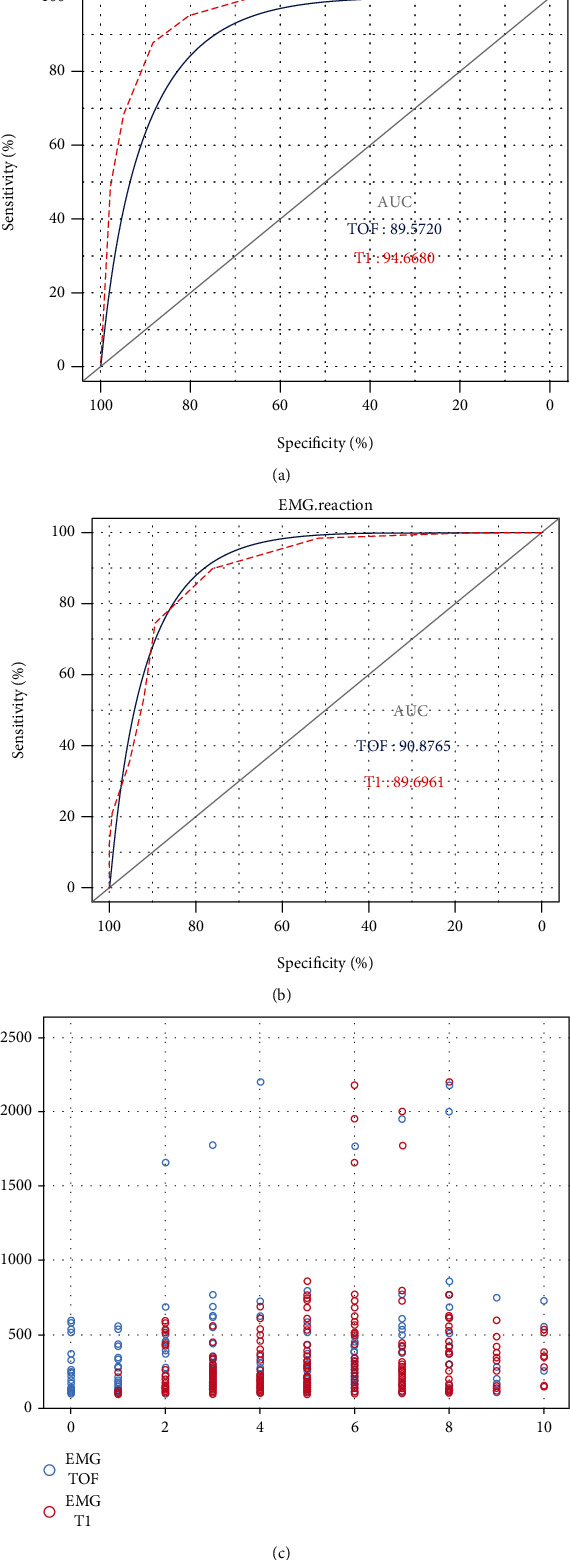
Methods: A total of 102 patients with the normal functioning preoperative facial nerve who required parotid tumour resection were included in this study. Facial nerve monitoring was conducted intraoperatively. The surgeon stimulated the facial nerve at different myorelaxation intervals at TOF% (T4/T1) and T1% (T1/T0) and recorded the responses and the amplitude of electromyogram (EMG). Body movements (BM) or patient-ventilator asynchrony (PVA) was recorded intraoperatively.
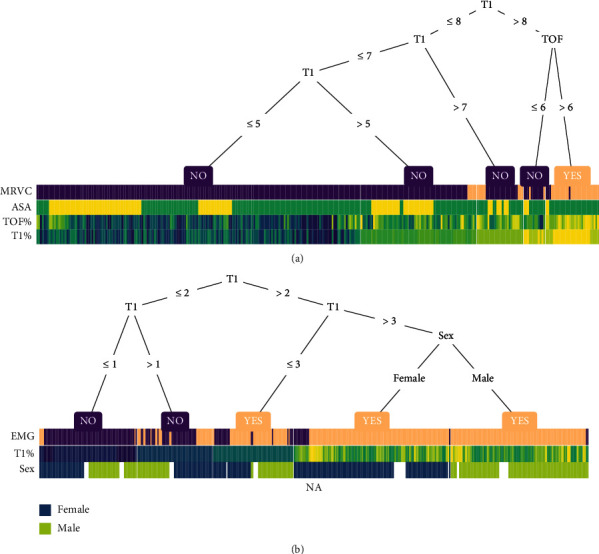
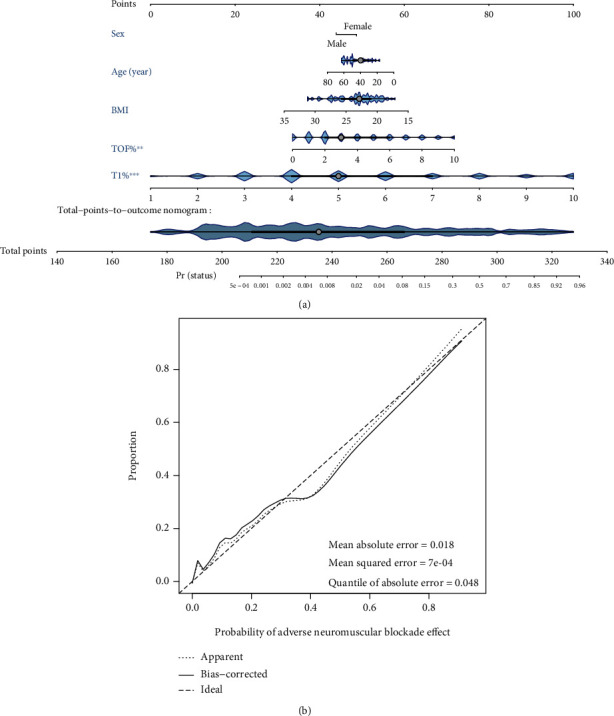
Results: In parotid tumour resection, T1% should be maintained at a range of 30 to 60% while TOF% should be maintained at a range of 20 to 30%. Analysis of the decision tree model for facial nerve monitoring suggests a partial muscle relaxation level of 30% < T1% ≤ 50% and TOF ≤ 60%. A nomogram prediction model, while incorporating factors such as sex, age, BMI, TOF%, and T1%, was constructed to predict the risk of BM/PVA during surgery, showing good predictive performance.
Conclusions: This study revealed an adequate level of neuromuscular blockade in intraoperative parotid tumour resection while conducting facial nerve monitoring. A visual nomogram prediction model was constructed to guide anaesthetists in improving the anaesthetic plan.
Copyright © 2021 Huimin Huang et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Schneck H. J., Rupreht J. Central anticholinergic syndrome (CAS) in anesthesia and intensive care. Acta Anaesthesiologica Belgica. 1989;40(3):219–228. - PubMed
-
- Amin A. M., Mohammad M. Y., Ibrahim M. F. Comparative study of neuromuscular blocking and hemodynamic effects of rocuronium and cisatracurium under sevoflurane or total intravenous anesthesia. Middle East Journal of Anaesthesiology. 2009;20(1):39–51. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
