

Exploiting DNA repair pathways for tumor sensitization, mitigation of resistance, and normal tissue protection in radiotherapy
- PMID: 34337349
- PMCID: PMC8323830
- DOI: 10.20517/cdr.2020.89
Exploiting DNA repair pathways for tumor sensitization, mitigation of resistance, and normal tissue protection in radiotherapy
Abstract
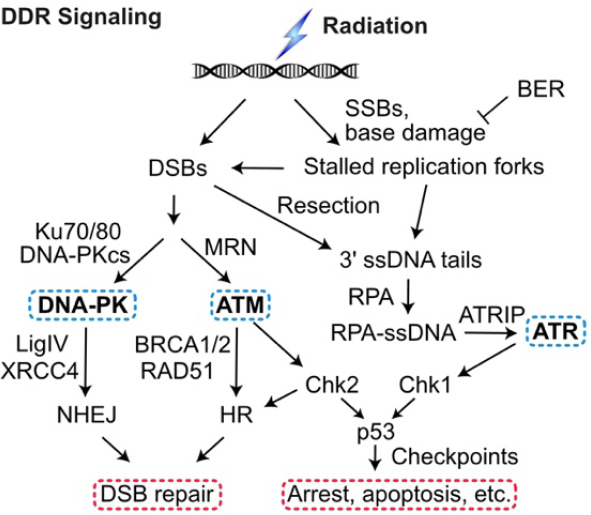
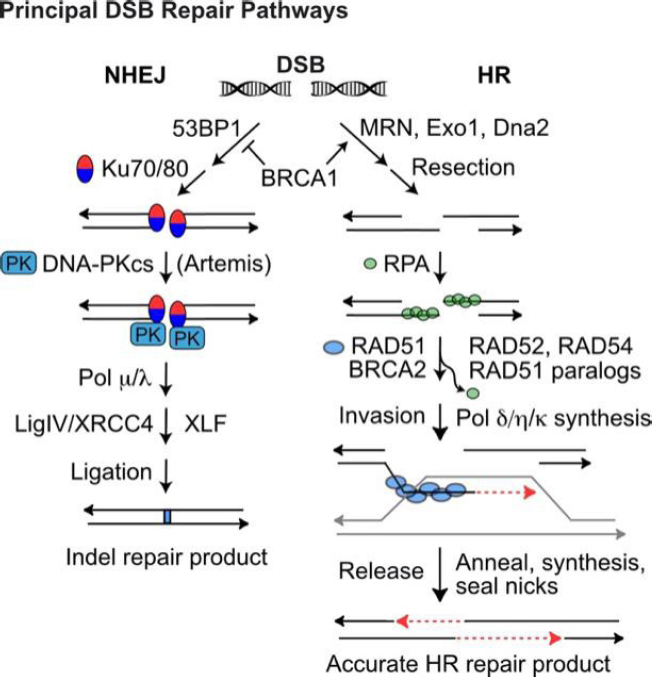
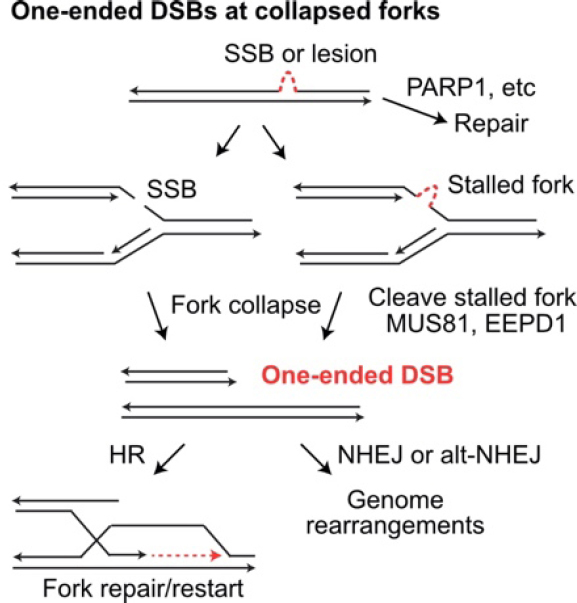
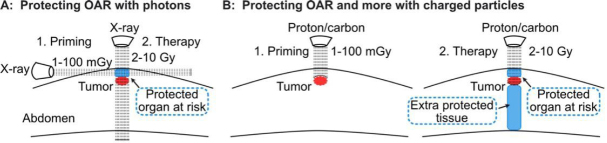
More than half of cancer patients are treated with radiotherapy, which kills tumor cells by directly and indirectly inducing DNA damage, including cytotoxic DNA double-strand breaks (DSBs). Tumor cells respond to these threats by activating a complex signaling network termed the DNA damage response (DDR). The DDR arrests the cell cycle, upregulates DNA repair, and triggers apoptosis when damage is excessive. The DDR signaling and DNA repair pathways are fertile terrain for therapeutic intervention. This review highlights strategies to improve therapeutic gain by targeting DDR and DNA repair pathways to radiosensitize tumor cells, overcome intrinsic and acquired tumor radioresistance, and protect normal tissue. Many biological and environmental factors determine tumor and normal cell responses to ionizing radiation and genotoxic chemotherapeutics. These include cell type and cell cycle phase distribution; tissue/tumor microenvironment and oxygen levels; DNA damage load and quality; DNA repair capacity; and susceptibility to apoptosis or other active or passive cell death pathways. We provide an overview of radiobiological parameters associated with X-ray, proton, and carbon ion radiotherapy; DNA repair and DNA damage signaling pathways; and other factors that regulate tumor and normal cell responses to radiation. We then focus on recent studies exploiting DSB repair pathways to enhance radiotherapy therapeutic gain.
Keywords: DNA double-strand break repair; DNA repair; cancer therapy; homologous recombination; non-homologous end-joining; radioprotection; radiosensitization.
Conflict of interest statement
Conflicts of interest All authors declared that there are no conflicts of interest.
Figures
References
-
- Halperin EC, Wazer DE, Perez CA, Brady LW. Perez & Brady’s Principles and Practice of Radiation Oncology. Lippincott Williams & Wilkins; 2018. p. 24.
Grants and funding
LinkOut - more resources
Full Text Sources