

Clinical Management of Children with a Congenital Solitary Functioning Kidney: Overview and Recommendations
- PMID: 34337499
- PMCID: PMC8317823
- DOI: 10.1016/j.euros.2021.01.003
Clinical Management of Children with a Congenital Solitary Functioning Kidney: Overview and Recommendations
Abstract
Context: A congenital solitary functioning kidney (cSFK) is a common developmental defect that predisposes to hypertension and chronic kidney disease (CKD) as a consequence of hyperfiltration. Every urologist takes care of patients with a cSFK, since some will need lifelong urological care or will come with clinical problems or questions to an adult urologist later in life.
Objective: We aim to provide clear recommendations for the initial clinical management and follow-up of children with a cSFK.
Evidence acquisition: PubMed and EMBASE were searched to identify relevant publications, which were combined with guidelines on related topics and expert opinion.
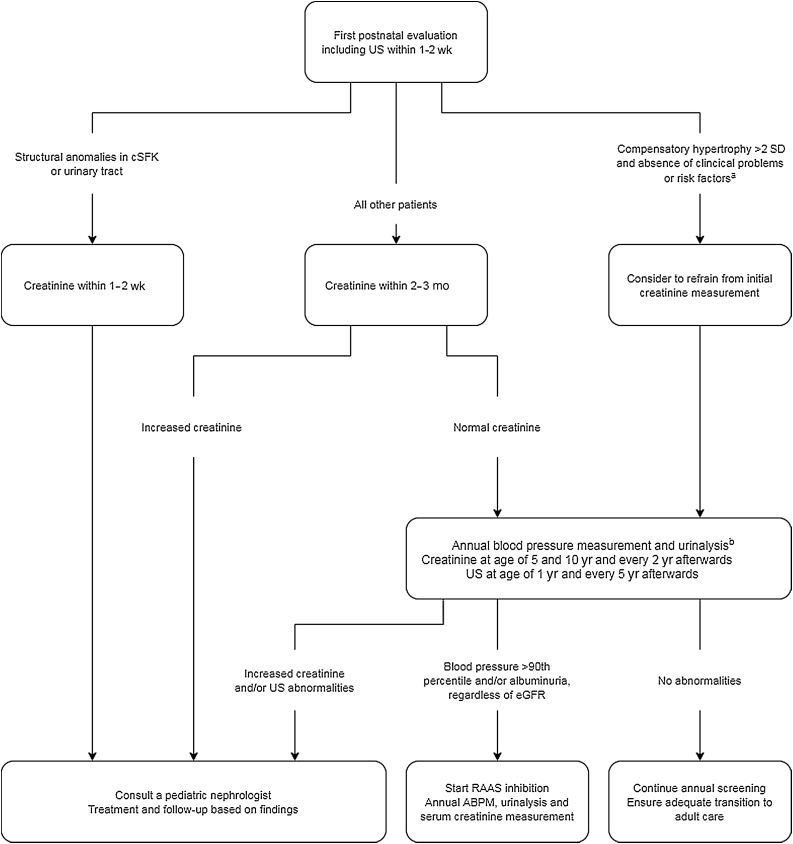
Evidence synthesis: Initially, cSFK diagnosis should be confirmed and risk factors for kidney injury should be identified using ultrasound. Although more research into early predictors of kidney injury is needed, additional congenital anomalies of the kidney or urinary tract and absence of compensatory kidney hypertrophy have repeatedly been associated with a worse prognosis. The role of voiding cystourethrography and antibiotic prophylaxis remains controversial, and is complicated by the exclusion of children with a cSFK from studies. A yearly follow-up for signs of kidney injury is recommended for children with a cSFK. As masked hypertension is prevalent, annual ambulatory blood pressure measurement should be considered. During puberty, an increasing incidence of kidney injury is seen, indicating that long-term follow-up is necessary. If signs of kidney injury are present, angiotensin converting enzyme inhibitors are the first-line drugs of choice.
Conclusions: This overview points to the urological and medical clinical aspects and long-term care guidance for children with a cSFK, who are at risk of hypertension and CKD. Monitoring for signs of kidney injury is therefore recommended throughout life. Large, prospective studies with long-term follow-up of clearly defined cohorts are still needed to facilitate more risk-based and individualized clinical management.
Patient summary: Many children are born with only one functioning kidney, which could lead to kidney injury later in life. Therefore, a kidney ultrasound is made soon after birth, and other investigations may be needed as well. Urologists taking care of patients with a solitary functioning kidney should realize the long-term clinical aspects, which might need medical management.
Keywords: Clinical management; Congenital anomalies of the kidney and urinary tract; Multicystic dysplastic kidney; Solitary functioning kidney; Unilateral renal agenesis.
© 2021 The Author(s).
Figures
References
-
- Hiraoka M., Tsukahara H., Ohshima Y., Kasuga K., Ishihara Y., Mayumi M. Renal aplasia is the predominant cause of congenital solitary kidneys. Kidney Int. 2002;61:1840–1844. - PubMed
-
- Schreuder M.F., Westland R., van Wijk J.A. Unilateral multicystic dysplastic kidney: a meta-analysis of observational studies on the incidence, associated urinary tract malformations and the contralateral kidney. Nephrol Dial Transplant. 2009;24:1810–1818. - PubMed
-
- Westland R., Schreuder M.F., Ket J.C., van Wijk J.A. Unilateral renal agenesis: a systematic review on associated anomalies and renal injury. Nephrol Dial Transpl. 2013;28:1844–1855. - PubMed
-
- Kim S., Chang Y., Lee Y.R. Solitary kidney and risk of chronic kidney disease. Eur J Epidemiol. 2019;34:879–888. - PubMed
-
- Sanna-Cherchi S., Ravani P., Corbani V. Renal outcome in patients with congenital anomalies of the kidney and urinary tract. Kidney Int. 2009;76:528–533. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
