

Comparative Survival Outcomes of High-risk Prostate Cancer Treated with Radical Prostatectomy or Definitive Radiotherapy Regimens
- PMID: 34337508
- PMCID: PMC8317873
- DOI: 10.1016/j.euros.2021.01.011
Comparative Survival Outcomes of High-risk Prostate Cancer Treated with Radical Prostatectomy or Definitive Radiotherapy Regimens
Abstract
Background: Observational data has indicated improved survival after radical prostatectomy (RP) compared with definitive radiotherapy (RT) in men with high-risk prostate cancer (PCa).
Objective: To compare PCa-specific mortality (PCSM) and overall mortality (OM) in men with high-risk PCa treated with RP or RT, providing information on target doses and fractionations.
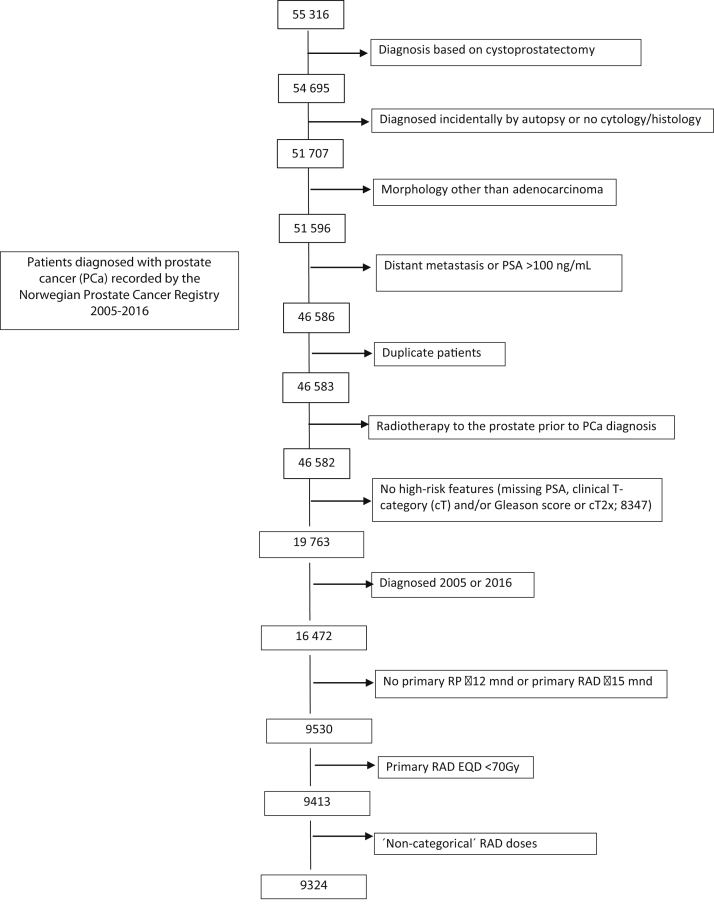
Design setting and participants: This is an observational study from the Cancer Registry of Norway. Patients were diagnosed with high-risk PCa during 2006-2015, treated with RP ≤12 mo or RT ≤15 mo after diagnosis, and stratified according to RP or RT modality; external beam radiotherapy (EBRT; 70-<74, 74-<78, or 78 Gy), hypofractionated RT or EBRT combined with brachytherapy (BT-RT).
Outcome measurements and statistical analysis: Competing risk and Kaplan-Meier methods estimated PCSM and OM, respectively. Multivariable Cox regression models evaluated hazard ratios (HRs) for PCSM and OM.
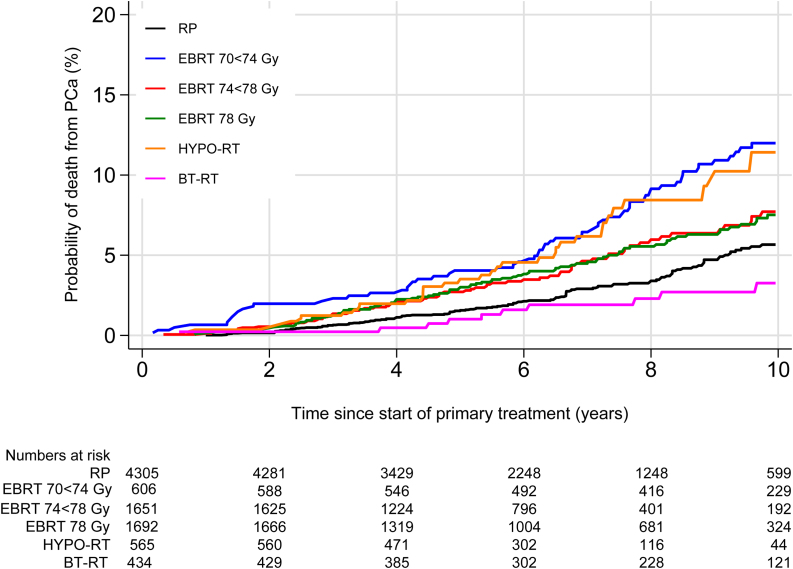
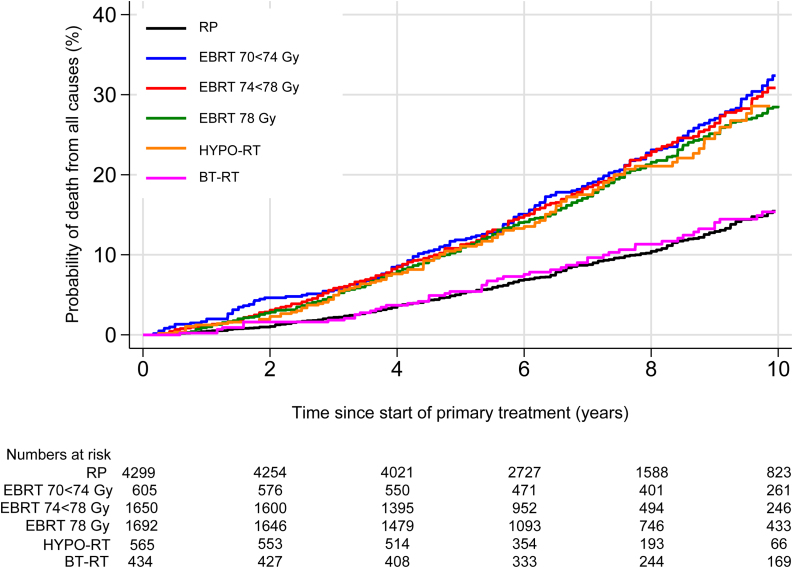
Results and limitations: In total, 9254 patients were included (RP 47%, RT 53%). RT patients were older, had poorer performance status and more unfavorable disease characteristics. With a median follow-up time of seven and eight yrs, the overall 10-yr PCSM was 7.2% (95% confidence interval [CI] 6.4-8.0) and OM was 22.9% (95% CI 21.8-24.1). Compared with RP, EBRT 70-<74 Gy was associated with increased (HR 1.88, 95% CI 1.33-2.65, p < 0.001) and BT-RT with decreased (HR 0.49, 95% CI 0.24-0.96, p = 0.039) 10-yr PCSM. Patients treated with EBRT 70-78 Gy had higher adjusted 10-yr OM than those treated with RP.
Conclusions: In men with high-risk PCa, treatment with EBRT <74 Gy was associated with increased adjusted 10-yr PCSM and OM, and BT-RT with decreased 10-yr PCSM, compared with RP.
Patient summary: In this study, we compared mortality after radical prostatectomy (RP) and radiotherapy (RT) in men with high-risk prostate cancer (PCa); the results suggest that men receiving lower-dose RT have higher, and patients receiving brachytherapy may have lower, risk of death from PCa than patients treated with prostatectomy.
Keywords: High risk; Mortality; Prostate cancer; Prostatectomy; Radiotherapy; Treatment.
© 2021 The Authors.
Figures
Similar articles
-
Ten-year survival after High-Dose-Rate Brachytherapy combined with External Beam Radiation Therapy in high-risk prostate cancer: A comparison with the Norwegian SPCG-7 cohort.Radiother Oncol. 2019 Mar;132:211-217. doi: 10.1016/j.radonc.2018.10.013. Epub 2018 Oct 30. Radiother Oncol. 2019. PMID: 30389241
-
Long-term Prostate Cancer-specific Mortality After Prostatectomy, Brachytherapy, External Beam Radiation Therapy, Hormonal Therapy, or Monitoring for Localized Prostate Cancer.Eur Urol. 2024 Jun;85(6):565-573. doi: 10.1016/j.eururo.2023.09.024. Epub 2023 Oct 17. Eur Urol. 2024. PMID: 37858454
-
External Beam Radiation Therapy With a Brachytherapy Boost Versus Radical Prostatectomy in Gleason Pattern 5 Prostate Cancer: A Population-Based Cohort Study.Int J Radiat Oncol Biol Phys. 2017 Aug 1;98(5):1045-1052. doi: 10.1016/j.ijrobp.2017.03.040. Epub 2017 Mar 31. Int J Radiat Oncol Biol Phys. 2017. PMID: 28721887
-
Benefits and Risks of Primary Treatments for High-risk Localized and Locally Advanced Prostate Cancer: An International Multidisciplinary Systematic Review.Eur Urol. 2020 May;77(5):614-627. doi: 10.1016/j.eururo.2020.01.033. Epub 2020 Mar 4. Eur Urol. 2020. PMID: 32146018
-
The efficacy and safety of radical prostatectomy and radiotherapy in high-risk prostate cancer: a systematic review and meta-analysis.World J Surg Oncol. 2020 Feb 24;18(1):42. doi: 10.1186/s12957-020-01824-9. World J Surg Oncol. 2020. PMID: 32093688 Free PMC article.
Cited by
-
Acute and long-term toxicity in primary hypofractionated external photon radiation therapy in patients with localized prostate cancer.World J Urol. 2024 Jan 20;42(1):41. doi: 10.1007/s00345-023-04714-3. World J Urol. 2024. PMID: 38244053 Free PMC article. Review.
-
Radiobiological analysis of preliminary results of a phase II study of pelvic hypofractionated and accelerated radiotherapy for high-risk prostate cancer patients.Radiat Oncol J. 2022 Jun;40(2):151-161. doi: 10.3857/roj.2021.01032. Epub 2022 Jun 20. Radiat Oncol J. 2022. PMID: 35796118 Free PMC article.
-
Comparing aerobic and resistance exercise emphasis during androgen deprivation and radiation therapy for prostate cancer: A randomised feasibility trial.Support Care Cancer. 2025 Jun 20;33(7):601. doi: 10.1007/s00520-025-09650-z. Support Care Cancer. 2025. PMID: 40540036 Free PMC article. Clinical Trial.
-
Geographic and socioeconomic variation in treatment of elderly prostate cancer patients in Norway - a national register-based study.Res Health Serv Reg. 2024 May 15;3(1):8. doi: 10.1007/s43999-024-00044-y. Res Health Serv Reg. 2024. PMID: 39177854 Free PMC article.
-
Comparison of Clinical Outcomes of Radical Prostatectomy versus IMRT with Long-Term Hormone Therapy for Relatively Young Patients with High- to Very High-Risk Localized Prostate Cancer.Cancers (Basel). 2021 Nov 28;13(23):5986. doi: 10.3390/cancers13235986. Cancers (Basel). 2021. PMID: 34885096 Free PMC article.
References
-
- Fossa S.D., Wiklund F., Klepp O. Ten- and 15-yr prostate cancer-specific mortality in patients with nonmetastatic locally advanced or aggressive intermediate prostate cancer, randomized to lifelong endocrine treatment alone or combined with radiotherapy: final results of the Scandinavian Prostate Cancer Group-7. Eur Urol. 2016;70:684–691. - PubMed
-
- Mottet N., Bellmunt J., Bolla M. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2017;71:618–629. - PubMed
-
- Moris L., Cumberbatch M.G., Van den Broeck T. Benefits and risks of primary treatments for high-risk localized and locally advanced prostate cancer: an international multidisciplinary systematic review. Eur Urol. 2020;77:614–627. - PubMed
-
- Wallis C.J.D., Saskin R., Choo R. Surgery versus radiotherapy for clinically-localized prostate cancer: a systematic review and meta-analysis. Eur Urol. 2016;70:21–30. - PubMed
LinkOut - more resources
Full Text Sources
