

Performance of crisis standards of care guidelines in a cohort of critically ill COVID-19 patients in the United States
- PMID: 34337554
- PMCID: PMC8316067
- DOI: 10.1016/j.xcrm.2021.100376
Performance of crisis standards of care guidelines in a cohort of critically ill COVID-19 patients in the United States
Abstract
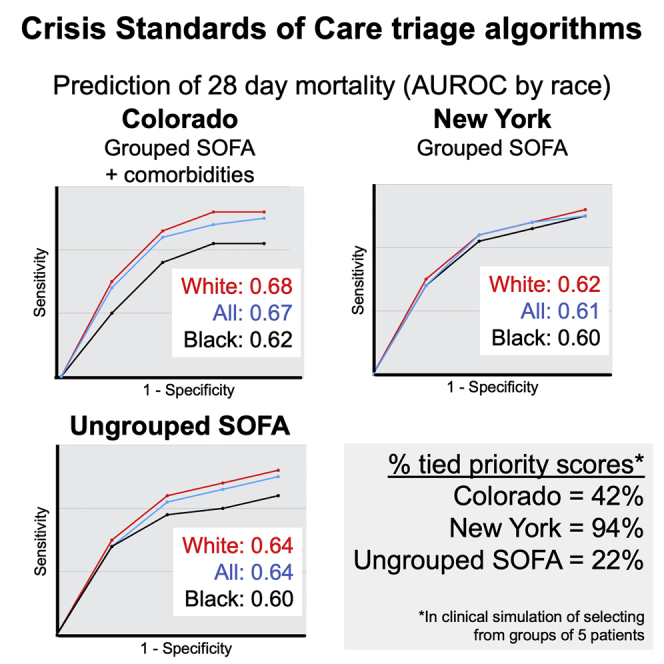
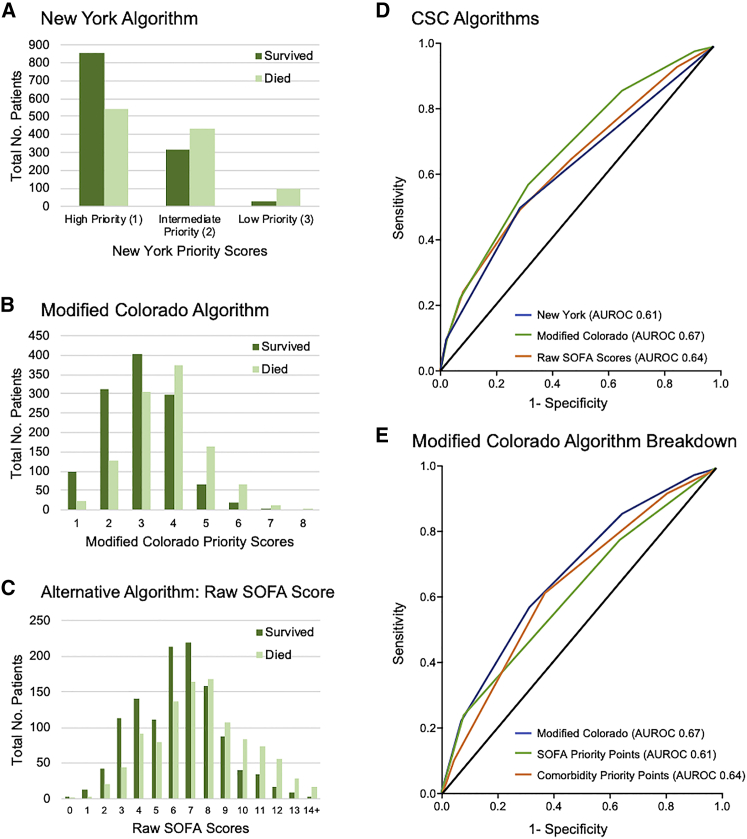
Many US states published crisis standards of care (CSC) guidelines for allocating scarce critical care resources during the COVID-19 pandemic. However, the performance of these guidelines in maximizing their population benefit has not been well tested. In 2,272 adults with COVID-19 requiring mechanical ventilation drawn from the Study of the Treatment and Outcomes in Critically Ill Patients with COVID-19 (STOP-COVID) multicenter cohort, we test the following three approaches to CSC algorithms: Sequential Organ Failure Assessment (SOFA) scores grouped into ranges, SOFA score ranges plus comorbidities, and a hypothetical approach using raw SOFA scores not grouped into ranges. We find that area under receiver operating characteristic (AUROC) curves for all three algorithms demonstrate only modest discrimination for 28-day mortality. Adding comorbidity scoring modestly improves algorithm performance over SOFA scores alone. The algorithm incorporating comorbidities has modestly worse predictive performance for Black compared to white patients. CSC algorithms should be empirically examined to refine approaches to the allocation of scarce resources during pandemics and to avoid potential exacerbation of racial inequities.
Keywords: ARDS; COVID-19; acute respiratory distress syndrome; crisis standards of care; critical care; intensive care; medical ethics; triage.
© 2021 The Author(s).
Conflict of interest statement
The authors have no conflicts of interest relevant to this work. For unrelated work, the authors have the following disclosures: S.P.K. served as a consultant for Resolve to Save Lives and has previously led a partnership on multiple chronic conditions at the Icahn School of Medicine at Mount Sinai with Teva Pharmaceuticals. W.B.F. serves as a consultant for Alosa Health and Aetion. He also received an honorarium for a presentation to Blue Cross Blue Shield of Massachusetts. E.Y.K. is a co-investigator in NCT04389671 (Windtree Therapeutics) testing lucinactant (surfactant-like treatment) in COVID-19 patients and received unrelated research funding from Bayer AG, N.I.H., the American Heart Association, the American Lung Association, and the American Thoracic Society.
Figures
Comment in
-
Allocation plans for crisis triage: How well would they actually work?Cell Rep Med. 2021 Sep 21;2(9):100379. doi: 10.1016/j.xcrm.2021.100379. Epub 2021 Sep 23. Cell Rep Med. 2021. PMID: 34585171 Free PMC article.
