

Polypharmacy and mortality association by chronic kidney disease status: The REasons for Geographic And Racial Differences in Stroke Study
- PMID: 34339112
- PMCID: PMC8328192
- DOI: 10.1002/prp2.823
Polypharmacy and mortality association by chronic kidney disease status: The REasons for Geographic And Racial Differences in Stroke Study
Abstract
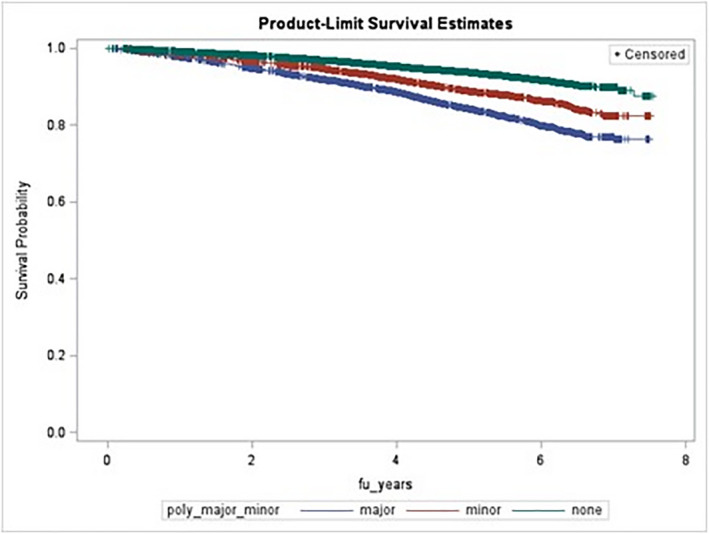
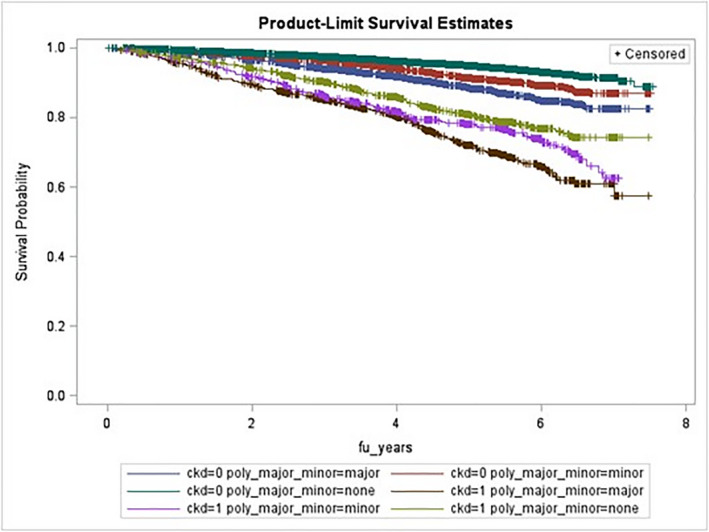
Many Americans take multiple medications simultaneously (polypharmacy). Polypharmacy's effects on mortality are uncertain. We endeavored to assess the association between polypharmacy and mortality in a large U.S. cohort and examine potential effect modification by chronic kidney disease (CKD) status. The REasons for Geographic And Racial Differences in Stroke cohort data (n = 29 627, comprised of U.S. black and white adults) were used. During a baseline home visit, pill bottle inspections ascertained medications used in the previous 2 weeks. Polypharmacy status (major [≥8 ingredients], minor [6-7 ingredients], and none [0-5 ingredients]) was determined by counting the total number of generic ingredients. Cox models (time-on-study and age-time-scale methods) assessed the association between polypharmacy and mortality. Alternative models examined confounding by indication and possible effect modification by CKD. Over 4.9 years median follow-up, 2538 deaths were observed. Major polypharmacy was associated with increased mortality in all models, with hazard ratios and 95% confidence intervals ranging from 1.22 (1.07-1.40) to 2.35 (2.15-2.56), with weaker associations in more adjusted models. Minor polypharmacy was associated with mortality in some, but not all, models. The polypharmacy-mortality association did not differ by CKD status. While residual confounding by indication cannot be excluded, in this large American cohort, major polypharmacy was consistently associated with mortality.
Keywords: REGARDS cohort study; chronic kidney disease; epidemiology; mortality; polypharmacy.
© 2021 The Authors. Pharmacology Research & Perspectives published by British Pharmacological Society and American Society for Pharmacology and Experimental Therapeutics and John Wiley & Sons Ltd.
Figures
References
-
- US FDA . Drug Applications for Over‐the‐Counter Drugs. 2010. http://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredeveloped.... Accessed July 29, 2012.
-
- Physician Desk Reference: For Nonprescription Drugs, Dietary Supplements, and Herbs. Thomson Healthcare; 2007.
-
- Hughes CM, McElnay J, Fleming GF. Benefits and risks of self medication. Drug Saf. 2001;24:1027‐1037. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
