

Menopausal hormone therapy and women's health: An umbrella review
- PMID: 34339416
- PMCID: PMC8366967
- DOI: 10.1371/journal.pmed.1003731
Menopausal hormone therapy and women's health: An umbrella review
Abstract
Background: There remains uncertainty about the impact of menopausal hormone therapy (MHT) on women's health. A systematic, comprehensive assessment of the effects on multiple outcomes is lacking. We conducted an umbrella review to comprehensively summarize evidence on the benefits and harms of MHT across diverse health outcomes.
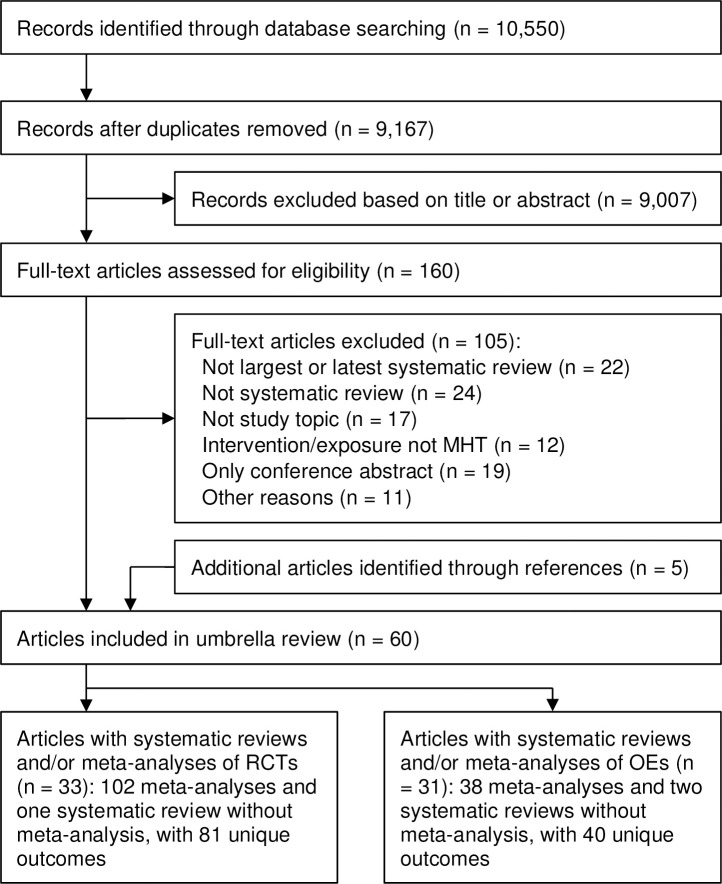
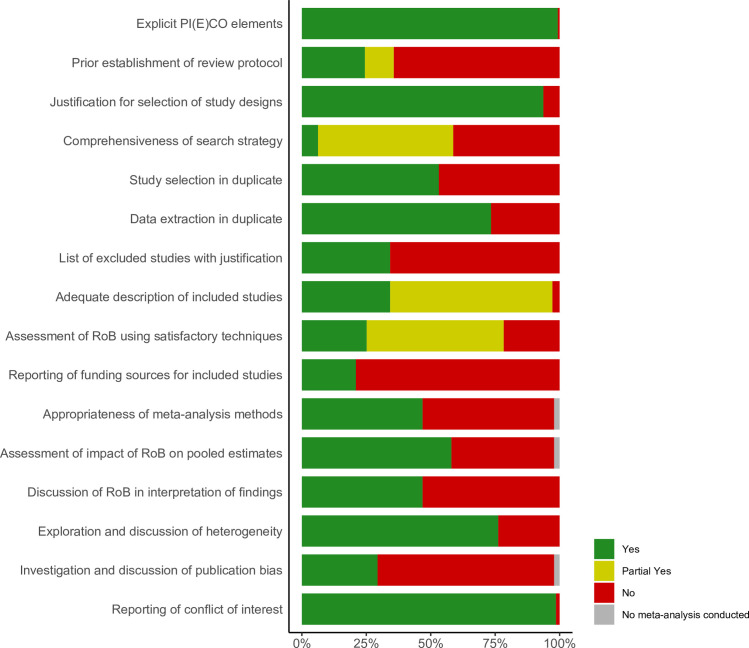
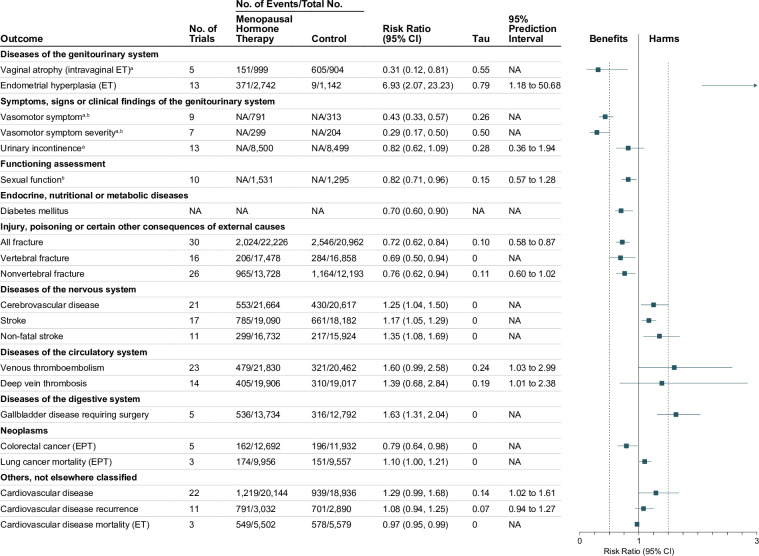
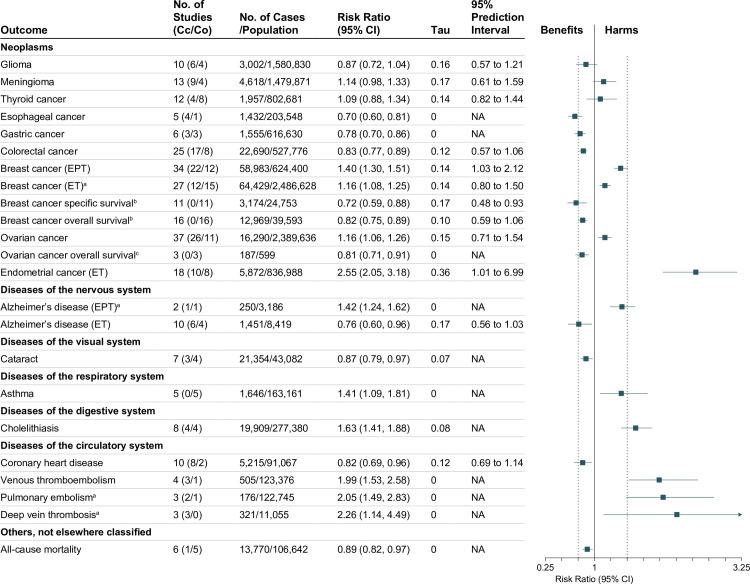
Methods and findings: We searched MEDLINE, EMBASE, and 10 other databases from inception to November 26, 2017, updated on December 17, 2020, to identify systematic reviews or meta-analyses of randomized controlled trials (RCTs) and observational studies investigating effects of MHT, including estrogen-alone therapy (ET) and estrogen plus progestin therapy (EPT), in perimenopausal or postmenopausal women in all countries and settings. All health outcomes in previous systematic reviews were included, including menopausal symptoms, surrogate endpoints, biomarkers, various morbidity outcomes, and mortality. Two investigators independently extracted data and assessed methodological quality of systematic reviews using the updated 16-item AMSTAR 2 instrument. Random-effects robust variance estimation was used to combine effect estimates, and 95% prediction intervals (PIs) were calculated whenever possible. We used the term MHT to encompass ET and EPT, and results are presented for MHT for each outcome, unless otherwise indicated. Sixty systematic reviews were included, involving 102 meta-analyses of RCTs and 38 of observational studies, with 102 unique outcomes. The overall quality of included systematic reviews was moderate to poor. In meta-analyses of RCTs, MHT was beneficial for vasomotor symptoms (frequency: 9 trials, 1,104 women, risk ratio [RR] 0.43, 95% CI 0.33 to 0.57, p < 0.001; severity: 7 trials, 503 women, RR 0.29, 95% CI 0.17 to 0.50, p = 0.002) and all fracture (30 trials, 43,188 women, RR 0.72, 95% CI 0.62 to 0.84, p = 0.002, 95% PI 0.58 to 0.87), as well as vaginal atrophy (intravaginal ET), sexual function, vertebral and nonvertebral fracture, diabetes mellitus, cardiovascular mortality (ET), and colorectal cancer (EPT), but harmful for stroke (17 trials, 37,272 women, RR 1.17, 95% CI 1.05 to 1.29, p = 0.027) and venous thromboembolism (23 trials, 42,292 women, RR 1.60, 95% CI 0.99 to 2.58, p = 0.052, 95% PI 1.03 to 2.99), as well as cardiovascular disease incidence and recurrence, cerebrovascular disease, nonfatal stroke, deep vein thrombosis, gallbladder disease requiring surgery, and lung cancer mortality (EPT). In meta-analyses of observational studies, MHT was associated with decreased risks of cataract, glioma, and esophageal, gastric, and colorectal cancer, but increased risks of pulmonary embolism, cholelithiasis, asthma, meningioma, and thyroid, breast, and ovarian cancer. ET and EPT had opposite effects for endometrial cancer, endometrial hyperplasia, and Alzheimer disease. The major limitations include the inability to address the varying effects of MHT by type, dose, formulation, duration of use, route of administration, and age of initiation and to take into account the quality of individual studies included in the systematic reviews. The study protocol is publicly available on PROSPERO (CRD42017083412).
Conclusions: MHT has a complex balance of benefits and harms on multiple health outcomes. Some effects differ qualitatively between ET and EPT. The quality of available evidence is only moderate to poor.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: HC reports no conflicts specifically related to menopausal hormone therapy, and in the more general area of women’s health the following are declared: Grant/Research Support in AUB treatment: Bayer AG; TAP Pharmaceuticals, Preglem/Gedeon-Richter: PEARL IV (with no personal remuneration); Speaker bureau on AUB Treatment: Bayer AG, Preglem/Gedeon-Richter, Myovant (with no personal remuneration); Consultancy/Advisory Board on AUB Treatment: Bayer AG, Preglem/Gedeon-Richter, Vifor Pharma, Myovant (with no personal remuneration); Royalties from UpToDate: for an article on abnormal uterine bleeding (personal remuneration received). AS is an Academic Editor on PLOS Medicine’s editorial board. CL has co-developed extracellular vesicle-associated patents for putative clinical utilization and owns equity in Exocure Bioscience Inc. HK reports personal fees and non-financial support from AstraZeneca, personal fees from Chiesi Pharma AB, personal fees and non-financial support from Boehringer-Ingelheim, personal fees from Novartis, personal fees from Mundipharma, personal fees and non-financial support from Orion Pharma, personal fees from SanofiGenzyme, personal fees from GlaxoSmithKline, outside the submitted work. All other authors have declared that no competing interests exist.
Figures
References
-
- United Nations Population Division. World population prospects 2019. New York: United Nations Population Division; 2020. [cited 2020 Nov 27]. Available from: https://population.un.org/wpp/DataQuery/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
