

Epidemiology of anal human papillomavirus infection and high-grade squamous intraepithelial lesions in 29 900 men according to HIV status, sexuality, and age: a collaborative pooled analysis of 64 studies
- PMID: 34339628
- PMCID: PMC8408042
- DOI: 10.1016/S2352-3018(21)00108-9
Epidemiology of anal human papillomavirus infection and high-grade squamous intraepithelial lesions in 29 900 men according to HIV status, sexuality, and age: a collaborative pooled analysis of 64 studies
Abstract
Background: Robust age-specific estimates of anal human papillomavirus (HPV) and high-grade squamous intraepithelial lesions (HSIL) in men can inform anal cancer prevention efforts. We aimed to evaluate the age-specific prevalence of anal HPV, HSIL, and their combination, in men, stratified by HIV status and sexuality.
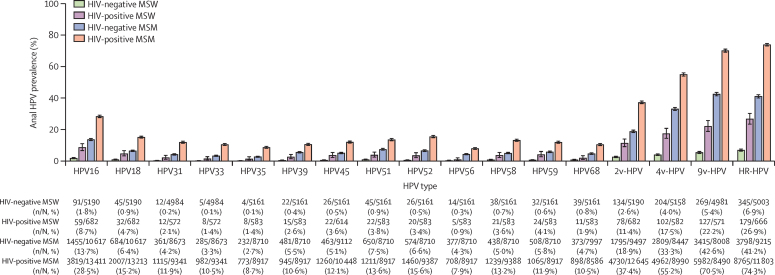
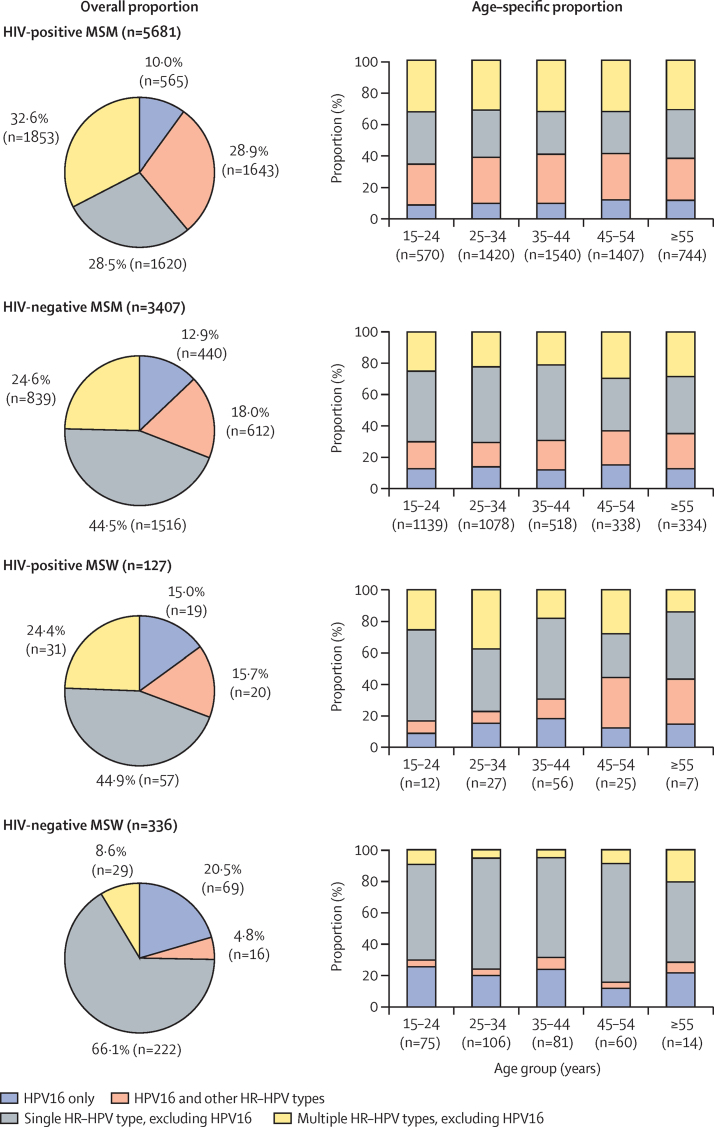
Methods: We did a systematic review for studies on anal HPV infection in men and a pooled analysis of individual-level data from eligible studies across four groups: HIV-positive men who have sex with men (MSM), HIV-negative MSM, HIV-positive men who have sex with women (MSW), and HIV-negative MSW. Studies were required to inform on type-specific HPV infection (at least HPV16), detected by use of a PCR-based test from anal swabs, HIV status, sexuality (MSM, including those who have sex with men only or also with women, or MSW), and age. Authors of eligible studies with a sample size of 200 participants or more were invited to share deidentified individual-level data on the above four variables. Authors of studies including 40 or more HIV-positive MSW or 40 or more men from Africa (irrespective of HIV status and sexuality) were also invited to share these data. Pooled estimates of anal high-risk HPV (HR-HPV, including HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68), and HSIL or worse (HSIL+), were compared by use of adjusted prevalence ratios (aPRs) from generalised linear models.
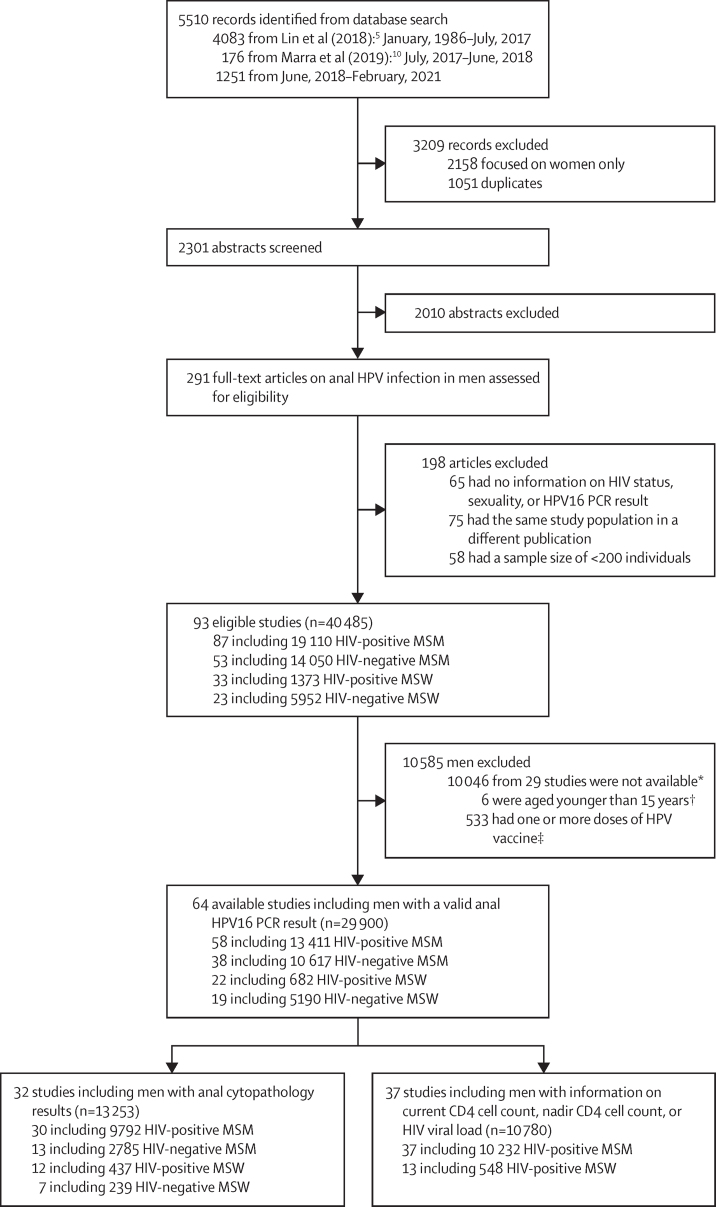
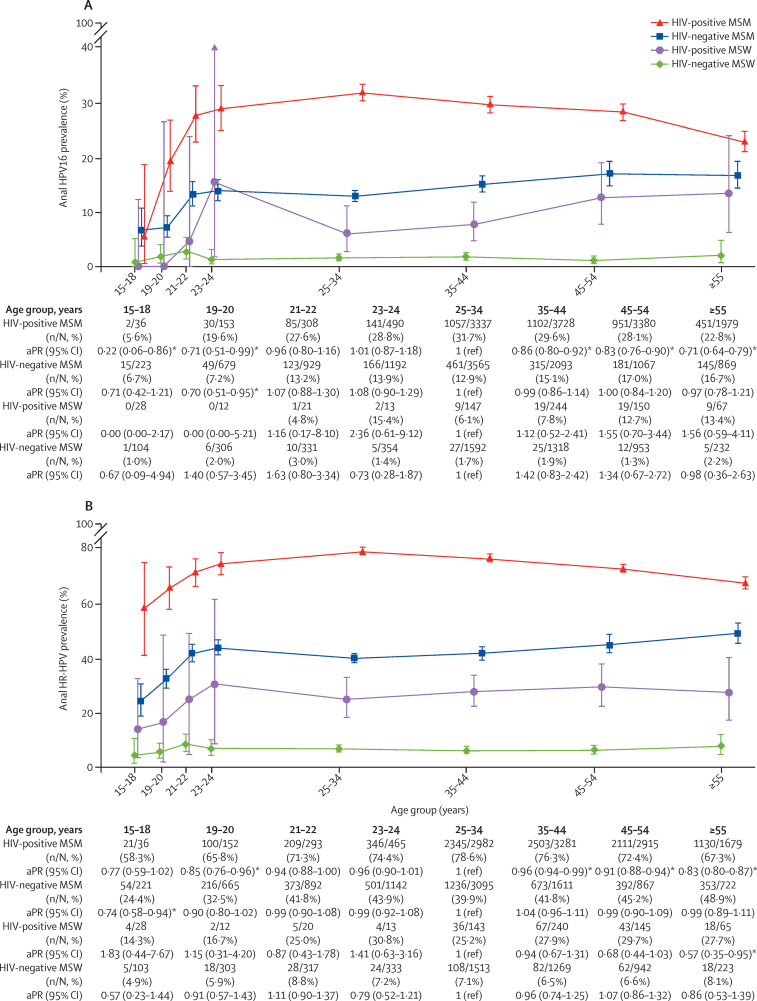
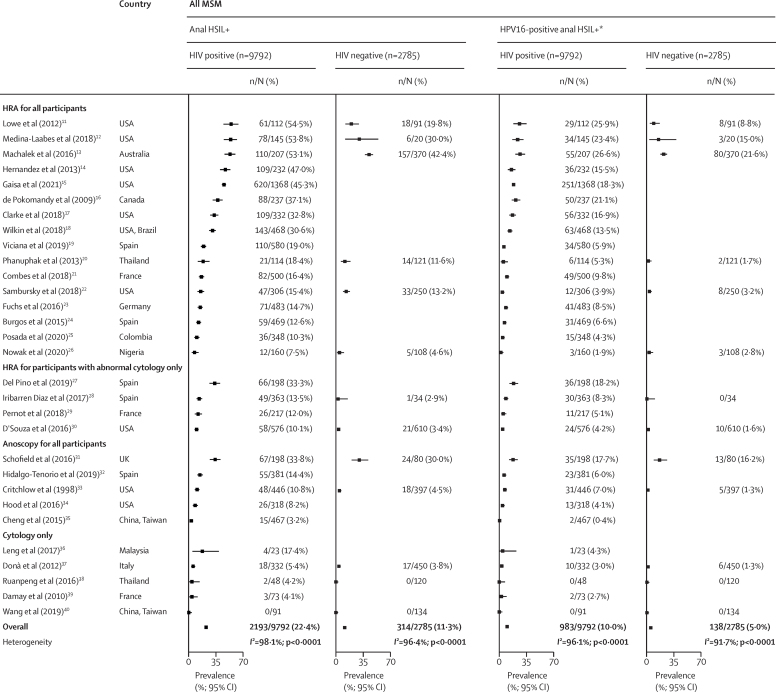
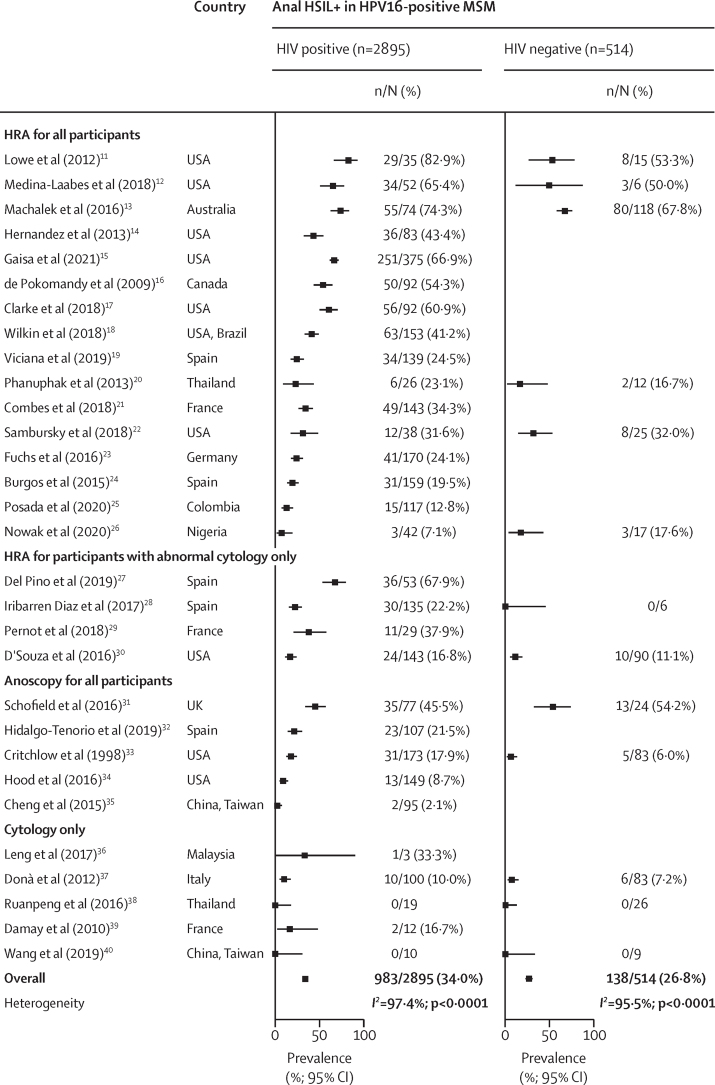
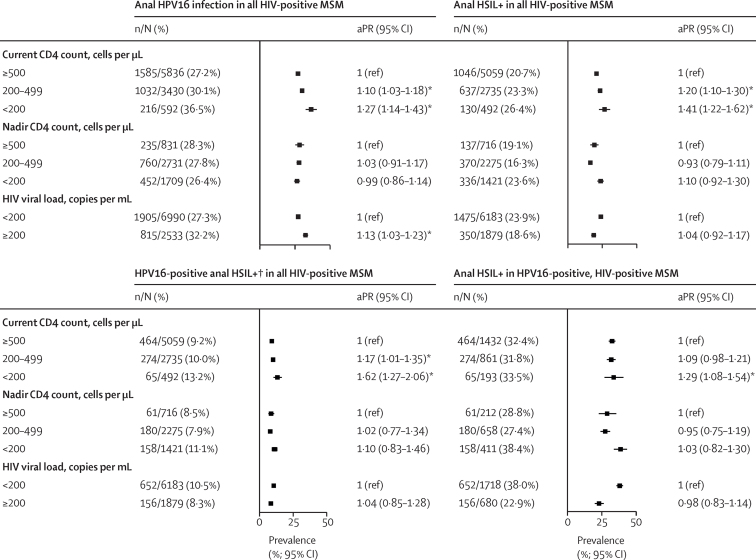
Findings: The systematic review identified 93 eligible studies, of which 64 contributed data on 29 900 men to the pooled analysis. Among HIV-negative MSW anal HPV16 prevalence was 1·8% (91 of 5190) and HR-HPV prevalence was 6·9% (345 of 5003); among HIV-positive MSW the prevalences were 8·7% (59 of 682) and 26·9% (179 of 666); among HIV-negative MSM they were 13·7% (1455 of 10 617) and 41·2% (3798 of 9215), and among HIV-positive MSM 28·5% (3819 of 13 411) and 74·3% (8765 of 11 803). In HIV-positive MSM, HPV16 prevalence was 5·6% (two of 36) among those age 15-18 years and 28·8% (141 of 490) among those age 23-24 years (ptrend=0·0091); prevalence was 31·7% (1057 of 3337) among those age 25-34 years and 22·8% (451 of 1979) among those age 55 and older (ptrend<0·0001). HPV16 prevalence in HIV-negative MSM was 6·7% (15 of 223) among those age 15-18 and 13·9% (166 of 1192) among those age 23-24 years (ptrend=0·0076); the prevalence plateaued thereafter (ptrend=0·72). Similar age-specific patterns were observed for HR-HPV. No significant differences for HPV16 or HR-HPV were found by age for either HIV-positive or HIV-negative MSW. HSIL+ detection ranged from 7·5% (12 of 160) to 54·5% (61 of 112) in HIV-positive MSM; after adjustment for heterogeneity, HIV was a significant predictor of HSIL+ (aPR 1·54, 95% CI 1·36-1·73), HPV16-positive HSIL+ (1·66, 1·36-2·03), and HSIL+ in HPV16-positive MSM (1·19, 1·04-1·37). Among HPV16-positive MSM, HSIL+ prevalence increased with age.
Interpretation: High anal HPV prevalence among young HIV-positive and HIV-negative MSM highlights the benefits of gender-neutral HPV vaccination before sexual activity over catch-up vaccination. HIV-positive MSM are a priority for anal cancer screening research and initiatives targeting HPV16-positive HSIL+.
Funding: International Agency for Research on Cancer.
© 2021 World Health Organization; licensee Elsevier. This is an Open Access article published under the CC BY-NC-ND 3.0 IGO license.
Conflict of interest statement
Declaration of interests ARG received travel fees from Merck & Co to participate in scientific advisory board meetings, and her institution has received grants for research from Merck & Co. SEH is funded by the US National Institutes of Health and the Bill & Melinda Gates Foundation outside the submitted work; and is a consultant for In Bios and a grant reviewer for US National Institutes of Health Study Section outside the submitted work. SEG received an investigator-initiated grant from Merck & Co, Inovio, and Medtronic outside the submitted work; consulting fees from THD America outside the submitted work; and payment as a speaker and financial support for attending meetings from Merck & Co outside the submitted work. MFSvdL received funds awarded to his institution from the AidsFonds charity and from Merck Sharpe & Dohme for participation on a data safety monitoring board or advisory board. KN is the recipient of a Miguel Servet research grant (CPII18/00033) from the Instituto de Salud Carlos III (Madrid, Spain) outside the submitted work. AGN received an investigator-initiated grant from Merck & Co in 2010–11 awarded to his institution at the time (Moffitt Cancer Center, Tampa, FL, USA) to assess the prevalence and incidence of anal HPV among men, allowing genotyping of samples (these data are included in the current Article); received travel fees from EUROGIN to present at their conferences; and received donated swabs and vials from COPAN. UW received grant support from the German Federal Ministry of Health for a study included in this report. EPFC is supported by an Australian National Health and Medical Research Council Emerging Leadership Investigator Grant (GNT1172873) outside the submitted work. YC received financial support from the Canadian Institutes of Health Research scholarship/studentship (CGS-D) outside the submitted work. YH received funding from the Natural Science Foundation of China International/Regional Research Collaboration Project (72061137007) and the Natural Science Foundation of China (81673232 and 82073574) outside the submitted work. GM received funding from US National Institutes of Health/National Cancer Institute outside the submitted work. APO received funds awarded to her institution from Aids Malignancy Consortium (2UM1CA121947–14) outside the submitted work; funds awarded to her institution from California-Mexico-Puerto Rico Partnership Center for Prevention of HPV-related Cancer in HIV-positive Populations (5U54CA242646–02) and from UPR/MDACC: Partnership for Excellence in Cancer Research (5U54-CA096297–17 and 5R21DE027226–02) outside the submitted work; and consulting fees and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, and educational events from Merck & Co outside the submitted work. HZ received funding awarded to Sun Yat-sen University from the Natural Science Foundation of China Excellent Young Scientists Fund (82022064), the Natural Science Foundation of China International/Regional Research Collaboration Project (72061137001), and the Precision Targeted Intervention Studies among High Risk Groups for HIV Prevention in China, National Science and Technology Major Project of China (2018ZX10721102) outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Advancing anal cancer prevention in men.Lancet HIV. 2021 Sep;8(9):e522-e523. doi: 10.1016/S2352-3018(21)00149-1. Epub 2021 Jul 30. Lancet HIV. 2021. PMID: 34339629 No abstract available.
References
-
- Islami F, Ferlay J, Lortet-Tieulent J, Bray F, Jemal A. International trends in anal cancer incidence rates. Int J Epidemiol. 2017;46:924–938. - PubMed
Uncited References
-
- Machalek DA, Poynten IM, Jin F. A composite cytology-histology endpoint allows a more accurate estimate of anal high-grade squamous intraepithelial lesion prevalence. Cancer Epidemiol Biomarkers Prev. 2016;25:1134–1143. - PubMed
-
- de Pokomandy A, Rouleau D, Ghattas G. Prevalence, clearance, and incidence of anal human papillomavirus infection in HIV-infected men: the HIPVIRG cohort study. J Infect Dis. 2009;199:965–973. - PubMed
