

Autoimmune Encephalitis Resembling Dementia Syndromes
- PMID: 34341093
- PMCID: PMC8362342
- DOI: 10.1212/NXI.0000000000001039
Autoimmune Encephalitis Resembling Dementia Syndromes
Abstract
Objective: As autoimmune encephalitis (AIE) can resemble neurodegenerative dementia syndromes, and patients do not always present as encephalitis, this study evaluates how frequently AIE mimics dementia and provides red flags for AIE in middle-aged and older patients.
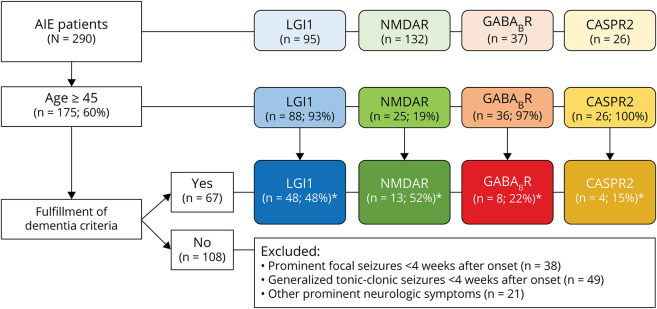
Methods: In this nationwide observational cohort study, patients with anti-leucine-rich glioma-inactivated 1 (LGI1), anti-NMDA receptor (NMDAR), anti-gamma-aminobutyric acid B receptor (GABABR), or anti-contactin-associated protein-like 2 (CASPR2) encephalitis were included. They had to meet 3 additional criteria: age ≥45 years, fulfillment of dementia criteria, and no prominent seizures early in the disease course (≤4 weeks).
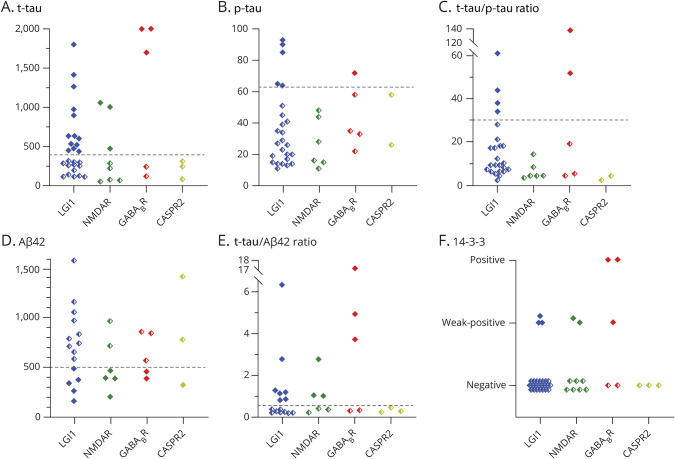
Results: Two-hundred ninety patients had AIE, of whom 175 were 45 years or older. Sixty-seven patients (38%) fulfilled criteria for dementia without prominent seizures early in the disease course. Of them, 42 had anti-LGI1 (48%), 13 anti-NMDAR (52%), 8 anti-GABABR (22%), and 4 anti-CASPR2 (15%) encephalitis. Rapidly progressive cognitive deterioration was seen in 48 patients (76%), whereas a neurodegenerative dementia syndrome was suspected in half (n = 33). In 17 patients (27%; 16/17 anti-LGI1), subtle seizures had been overlooked. Sixteen patients (25%) had neither inflammatory changes on brain MRI nor CSF pleocytosis. At least 1 CSF biomarker, often requested when dementia was suspected, was abnormal in 27 of 44 tested patients (61%), whereas 8 had positive 14-3-3 results (19%). Most patients (84%) improved after immunotherapy.
Conclusions: Red flags for AIE in patients with suspected dementia are: (1) rapidly progressive cognitive decline, (2) subtle seizures, and (3) abnormalities in ancillary testing atypical for neurodegeneration. Physicians should be aware that inflammatory changes are not always present in AIE, and that biomarkers often requested when dementia was suspected (including 14-3-3) can show abnormal results. Diagnosis is essential as most patients profit from immunotherapy.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- van Sonderen A, Thijs RD, Coenders EC, et al. . Anti-LGI1 encephalitis: clinical syndrome and long-term follow-up. Neurology. 2016;87(14):1449-1456. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials