

Mortality and predictors of acute kidney injury in adults: a hospital-based prospective observational study
- PMID: 34341369
- PMCID: PMC8329200
- DOI: 10.1038/s41598-021-94946-3
Mortality and predictors of acute kidney injury in adults: a hospital-based prospective observational study
Abstract
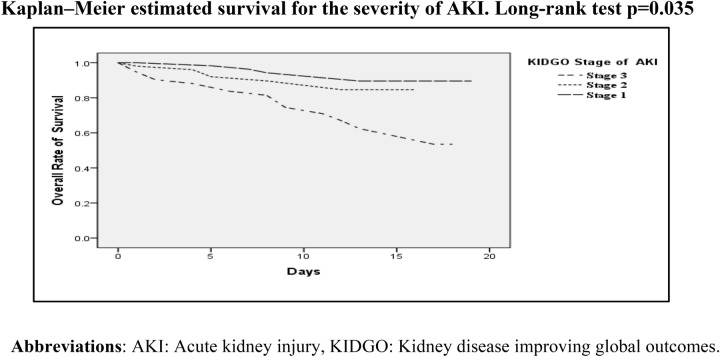
Acute kidney injury (AKI) is a major global public health problem. It is expensive to manage and associated with a high rate of prolonged hospitalization and in-hospital mortality. Little is known about the burden of acute kidney injury in moderate to low-income countries. We aim to assess predictors of in-hospital mortality among AKI patients admitted to the medical ward. We prospectively identified patients meeting kidney disease improving global outcomes (KIDGO) AKI definitions from April to August 2019. Patients with underlying CKD and patients hospitalized for less than 48 h were excluded. The Cox regression model was fitted to identify predictors of mortality and statistical significance was considered at the p-value of less than 0.05. A total of 203 patients were enrolled over 5 months. Out of this, 121(59.6%) were males, 58(28.6%) were aged greater than 60 years, and 141(69.5%) had community-acquired acute kidney injury. The most common causes of AKI were Hypovolemia 99(48.77%), Glomerulonephritis 51(25.11%), and sepsis 32(15.79%). The overall in-hospital mortality rate was 12.8%. Stage 3 AKI (AHR = 9.61, 95% CI 1.17-28.52, p = 0.035), duration of AKI (AHR = 7.04, 95% CI 1.37-36.08, p = 0.019), length of hospital stay (AHR = 0.19, 95% CI 0.05-0.73, p = 0.012), and hyperkalemia (AHR = 3.61, 95% CI 1.12-11.71, p = 0.032) were significantly associated with in-hospital mortality. There is a high rate of acute kidney injury-related in-hospital mortality in adult patients admitted to the medical ward. The severity of AKI, hyperkalemia duration of AKI, and a short length of hospital stay were predictors of 30-days in-hospital mortality. Most of the causes of AKI are preventable and patients may benefit from early identification and treatment of these reversible causes.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- KDIGO Clinical practice guideline for acute kidney injury. Off. J. Int. Soc. Nephrol. 2012;2(1):124–138.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
