

Salivary proteome of aphthous stomatitis reveals the participation of vitamin metabolism, nutrients, and bacteria
- PMID: 34341431
- PMCID: PMC8329211
- DOI: 10.1038/s41598-021-95228-8
Salivary proteome of aphthous stomatitis reveals the participation of vitamin metabolism, nutrients, and bacteria
Abstract
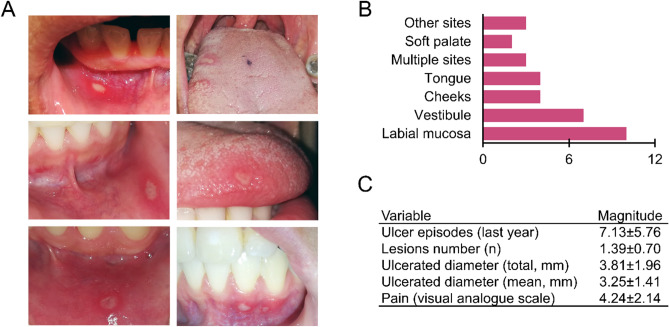
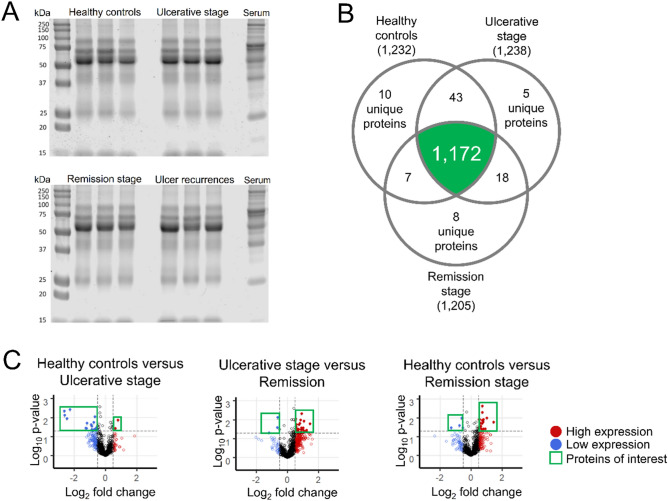
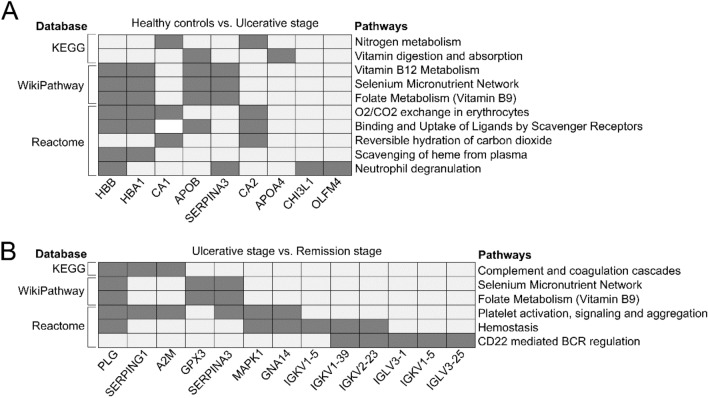
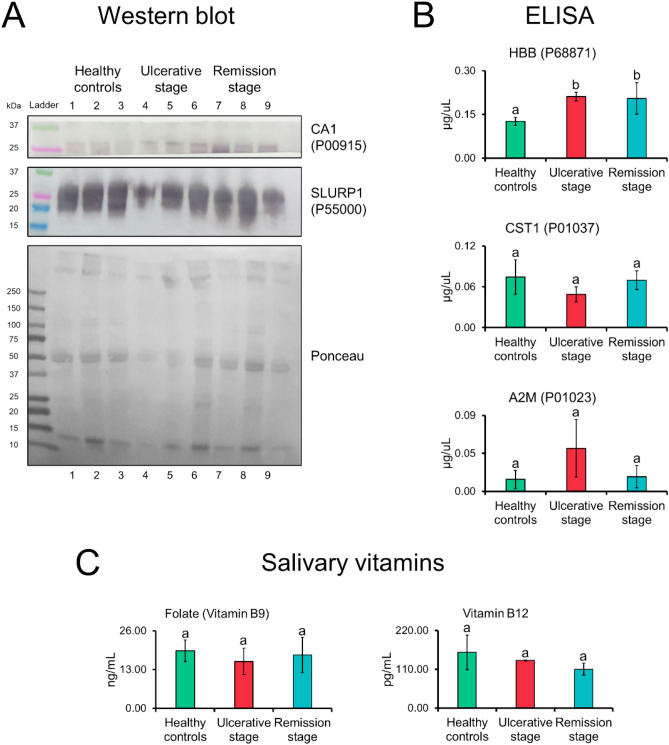
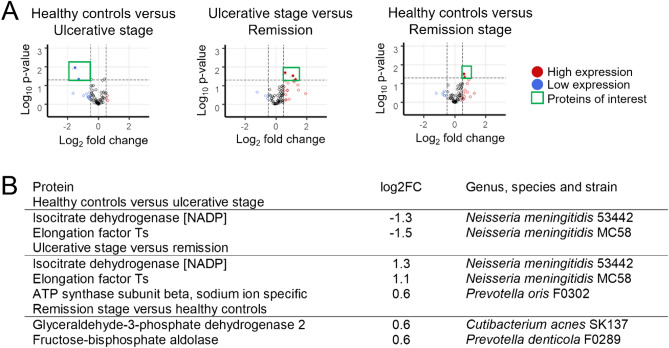
There are currently no preventative options for recurrent aphthous stomatitis, and the only available treatments are palliative. This is partly due to a poor understanding of its etiopathogenesis. In this case-control study, we characterized the salivary proteome of patients with recurrent aphthous stomatitis in the presence and absence of lesions. Through mass spectrometry-based proteomics and bioinformatics tools, we identified that the presence of oral ulcers is associated with several specific biological processes, including the metabolic pathways of vitamin B9, B12, nitrogen, selenium, and the bacterium Neisseria meningitidis. These changes occurred only in the presence of clinically visible lesions, and there were no relevant differences between patients in anatomical regions unaffected by ulcers. Additionally, using western blot and ELISA assays, we verified that carbonic anhydrase 1 (CA1) and hemoglobin subunit beta (HBB) proteins are highly expressed during the ulcerative and remission phases of recurrent aphthous stomatitis. Our results cumulatively support saliva as an indicator of the pathophysiological changes, which occur during the clinical course of lesions. From a clinical perspective, we suggest that recurrent aphthous stomatitis is a condition triggered by temporary biological changes in people with lesions.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Salivary proteins offer insights into keratinocyte death during aphthous stomatitis. A case-crossover study.BMC Oral Health. 2023 May 11;23(1):279. doi: 10.1186/s12903-023-02955-7. BMC Oral Health. 2023. PMID: 37170213 Free PMC article.
-
Salivary mucin MUC7 oligosaccharides in patients with recurrent aphthous stomatitis.Clin Oral Investig. 2015 Nov;19(8):2147-52. doi: 10.1007/s00784-015-1495-3. Epub 2015 Jun 9. Clin Oral Investig. 2015. PMID: 26051835 Clinical Trial.
-
Assessment of salivary and serum antioxidant vitamins and lipid peroxidation in patients with recurrent aphthous ulceration.Tohoku J Exp Med. 2005 Aug;206(4):305-12. doi: 10.1620/tjem.206.305. Tohoku J Exp Med. 2005. PMID: 15997201
-
Recurrent aphthous stomatitis. An update.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996 Feb;81(2):141-7. doi: 10.1016/s1079-2104(96)80403-3. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996. PMID: 8665304 Review.
-
Recurrent aphthous stomatitis: clinical characteristics and associated systemic disorders.Semin Cutan Med Surg. 1997 Dec;16(4):278-83. doi: 10.1016/s1085-5629(97)80017-x. Semin Cutan Med Surg. 1997. PMID: 9421219 Review.
Cited by
-
Expression of Salivary Ceramide Synthase 1 (CERS1) in Recurrent Aphthous Stomatitis (RAS): A Cross-Sectional Institutional Study.Cureus. 2023 Jul 9;15(7):e41597. doi: 10.7759/cureus.41597. eCollection 2023 Jul. Cureus. 2023. PMID: 37559835 Free PMC article.
-
Aphthous stomatitis - computational biology suggests external biotic stimulus and immunogenic cell death involved.BMC Oral Health. 2024 Sep 29;24(1):1154. doi: 10.1186/s12903-024-04917-z. BMC Oral Health. 2024. PMID: 39343890 Free PMC article.
-
Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis.Medicina (Kaunas). 2022 Jun 7;58(6):771. doi: 10.3390/medicina58060771. Medicina (Kaunas). 2022. PMID: 35744034 Free PMC article. Review.
References
-
- Rivera C. Insights into etiopathogenic and clinical features in 3RU oral diseases: An interesting and challenging research focus. J. Oral Res. 2017;6:35. doi: 10.17126/joralres.2017.012. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
