

Prefrontal cortex and depression
- PMID: 34341498
- PMCID: PMC8617037
- DOI: 10.1038/s41386-021-01101-7
Prefrontal cortex and depression
Erratum in
-
Correction: Prefrontal cortex and depression.Neuropsychopharmacology. 2022 Jan;47(2):609. doi: 10.1038/s41386-021-01160-w. Neuropsychopharmacology. 2022. PMID: 34413479 Free PMC article. No abstract available.
Abstract
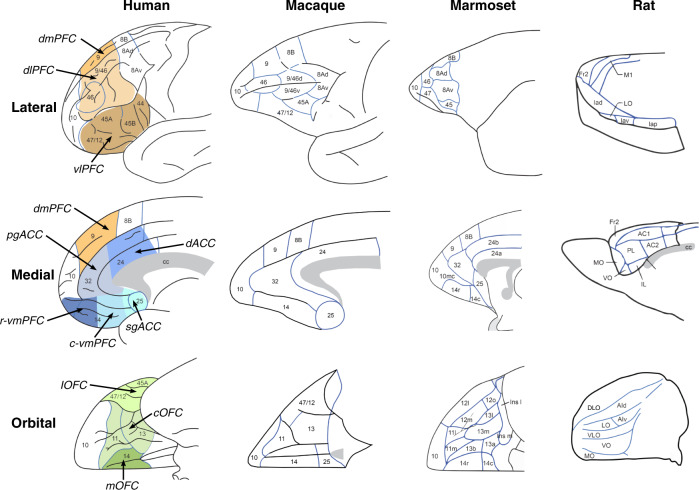
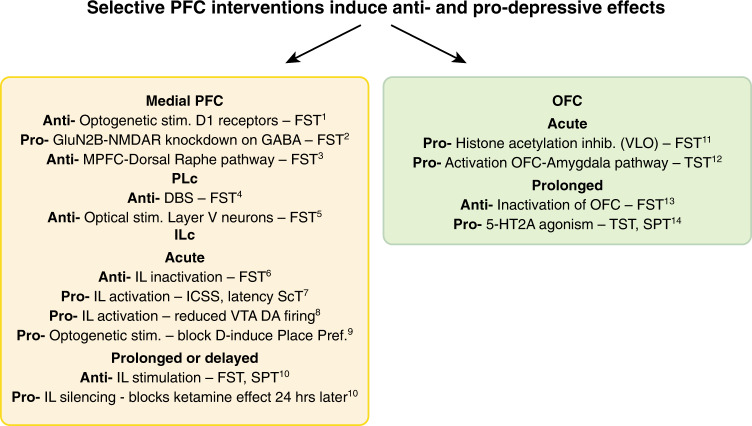
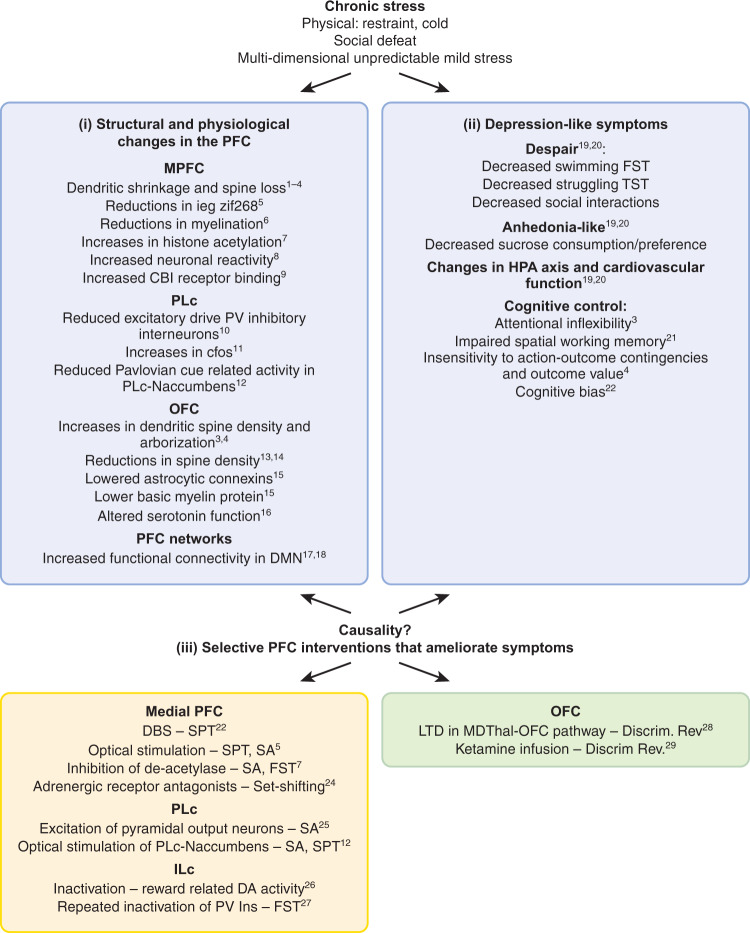
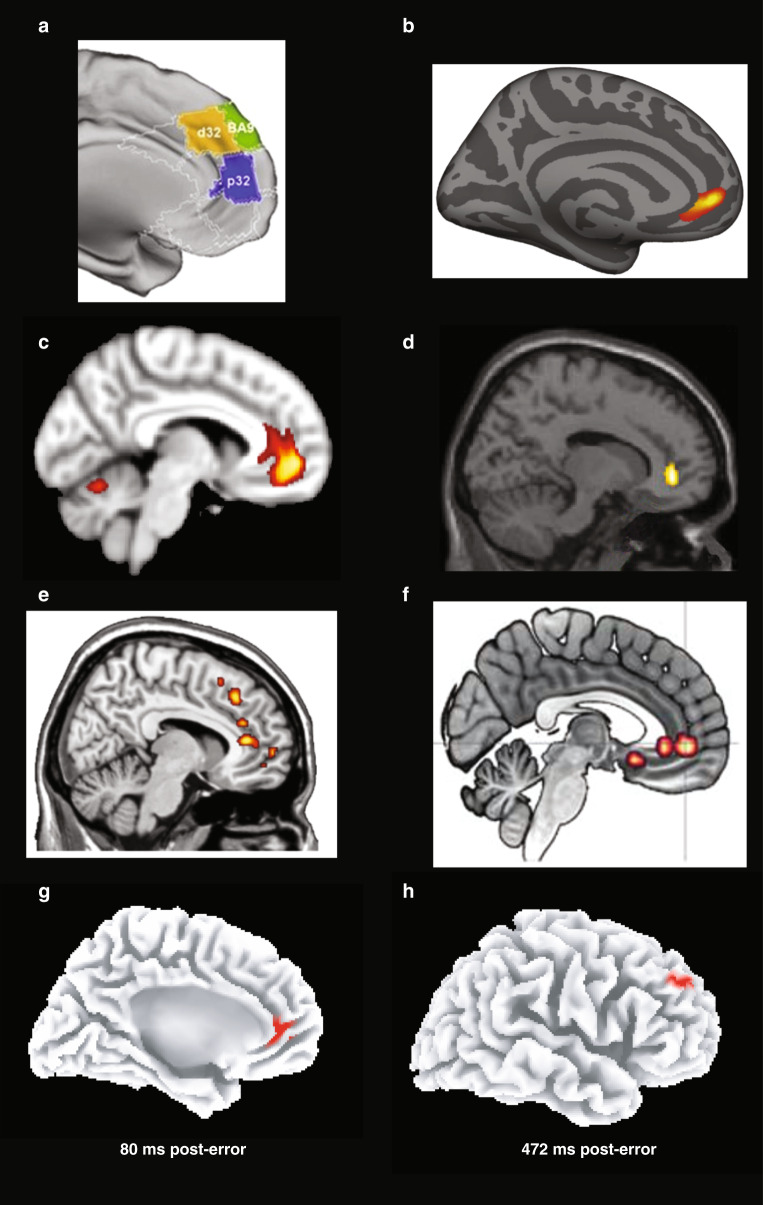
The prefrontal cortex (PFC) has emerged as one of the regions most consistently impaired in major depressive disorder (MDD). Although functional and structural PFC abnormalities have been reported in both individuals with current MDD as well as those at increased vulnerability to MDD, this information has not translated into better treatment and prevention strategies. Here, we argue that dissecting depressive phenotypes into biologically more tractable dimensions - negative processing biases, anhedonia, despair-like behavior (learned helplessness) - affords unique opportunities for integrating clinical findings with mechanistic evidence emerging from preclinical models relevant to depression, and thereby promises to improve our understanding of MDD. To this end, we review and integrate clinical and preclinical literature pertinent to these core phenotypes, while emphasizing a systems-level approach, treatment effects, and whether specific PFC abnormalities are causes or consequences of MDD. In addition, we discuss several key issues linked to cross-species translation, including functional brain homology across species, the importance of dissecting neural pathways underlying specific functional domains that can be fruitfully probed across species, and the experimental approaches that best ensure translatability. Future directions and clinical implications of this burgeoning literature are discussed.
© 2021. The Author(s), under exclusive licence to American College of Neuropsychopharmacology.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Wittchen HU, Jacobi F, Rehm J, Gustavsson A, Svensson M, Jönsson B, et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharmacol. 2011;21:655–79. - PubMed
-
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370:851–8. - PubMed
-
- Hyman SE. Can neuroscience be integrated into the DSM-V? Nat Rev Neurosci. 2007;8:725–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
