

A prospective study of dual-energy computed tomography for differentiating metastatic and non-metastatic lymph nodes of colorectal cancer
- PMID: 34341722
- PMCID: PMC8245958
- DOI: 10.21037/qims-20-3
A prospective study of dual-energy computed tomography for differentiating metastatic and non-metastatic lymph nodes of colorectal cancer
Abstract
Background: Colorectal cancer (CRC) is the third most common malignancy worldwide, and lymph node metastasis is considered to be a risk factor for local recurrence and a poor prognosis in colorectal cancer. However, there remains a lack of reliable and non-invasive biomarkers to identify the lymph node status of CRC patients preoperatively. The purpose of this study was to explore the ability of dual-energy computed tomography (DECT) to differentiate metastatic from non-metastatic lymph nodes in colorectal cancer.
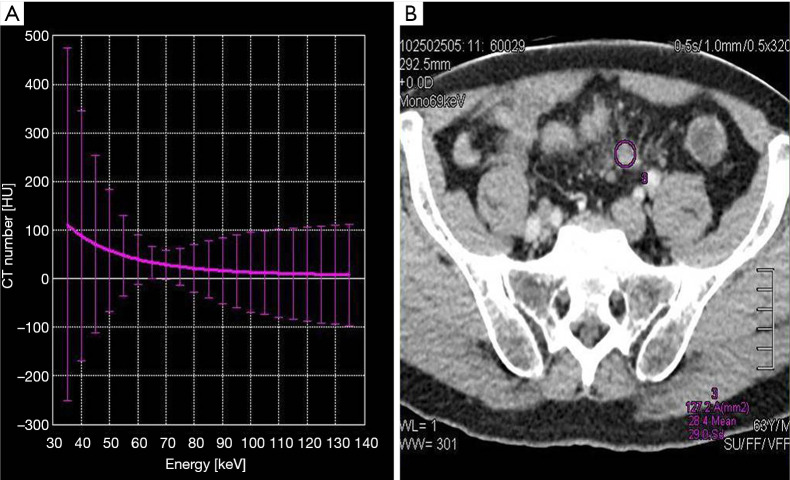
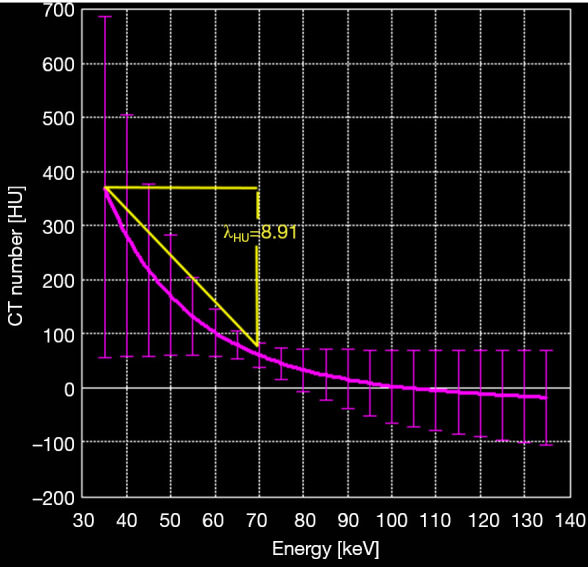
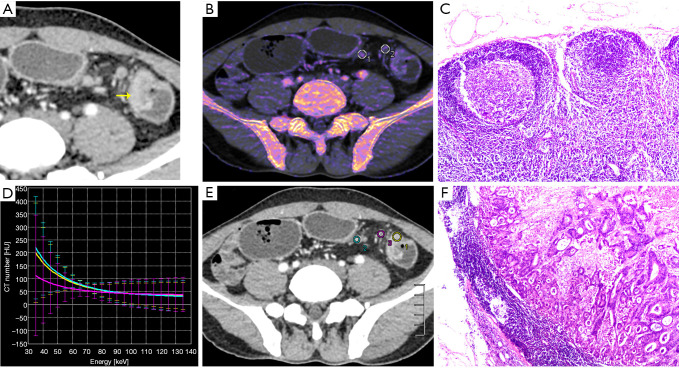
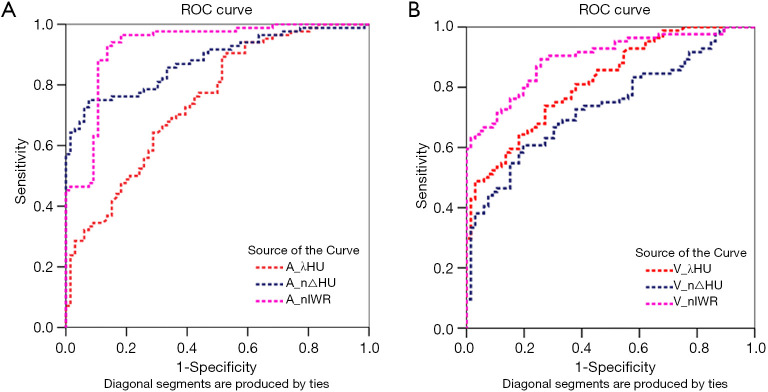
Methods: Seventy-one patients with primary colorectal cancer underwent contrast-enhanced dual-energy computed tomography imaging preoperatively. The colorectal specimen was scanned postoperatively, and lymph nodes were matched to the pathology report. The following dual-energy computed tomography quantitative parameters were analyzed: dual-energy curve slope value (λHU), standardized iodine concentration (n△HU), iodine water ratio (nIWR), electron density value (nρeff), and effective atom-number (nZ), based on metastatic and non-metastatic lymph node differentiation. Also, sensitivity and specificity analyses were performed using receiver operating characteristic curves.
Results: In all patients, one hundred and fifty lymph nodes, including 66 non-metastatic and 84 metastatic lymph nodes, were matched using the radiological-pathological correlation. Metastatic nodes had significantly greater λHU, n△HU, and nIWR values than non-metastatic nodes in both the arterial and venous phases (P<0.01). The area under curve (AUC), sensitivity, and specificity were 0.80, 80%, and 66% for λHU; 0.86, 70%, and 95% for n△HU; and 0.88, 71%, and 95% for nIWR in the arterial phase. There was no significant difference in electron density and effective Z values between metastatic and non-metastatic lymph nodes.
Conclusions: DECT quantitative parameters may help differentiate between metastatic and normal lymph nodes in patients with CRC.
Keywords: Computed tomography; colorectal cancer (CRC); dual-energy CT (DECT); lymph node; staging.
2021 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE (International Committee of Medical Journal Editors) uniform disclosure form (available at http://dx.doi.org/10.21037/qims-20-3). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Dual-Energy Computed Tomography in Detecting and Predicting Lymph Node Metastasis in Malignant Tumor Patients: A Comprehensive Review.Diagnostics (Basel). 2024 Feb 9;14(4):377. doi: 10.3390/diagnostics14040377. Diagnostics (Basel). 2024. PMID: 38396416 Free PMC article. Review.
-
Diagnosing cervical lymph node metastasis in oral squamous cell carcinoma based on third-generation dual-source, dual-energy computed tomography.Eur Radiol. 2023 Jan;33(1):162-171. doi: 10.1007/s00330-022-09033-6. Epub 2022 Sep 7. Eur Radiol. 2023. PMID: 36070090 Free PMC article.
-
[Comparative imaging study of mediastinal lymph node from pre-surgery dual energy CT versus post-surgeron verifications in non-small cell lung cancer patients].Beijing Da Xue Xue Bao Yi Xue Ban. 2020 Aug 18;52(4):730-737. doi: 10.19723/j.issn.1671-167X.2020.04.026. Beijing Da Xue Xue Bao Yi Xue Ban. 2020. PMID: 32773811 Free PMC article. Chinese.
-
Assessment of lymph node metastases in patients with ovarian high-grade serous carcinoma: Incremental diagnostic value of dual-energy CT combined with morphologic parameters.Eur J Radiol. 2025 Jun;187:112107. doi: 10.1016/j.ejrad.2025.112107. Epub 2025 Apr 9. Eur J Radiol. 2025. PMID: 40222185
-
The Diagnostic Impact of Contrast-Enhanced Computed Tomography (CECT) in Evaluating Lymph Node Involvement in Colorectal Cancer: A Comprehensive Review.Cureus. 2024 Jun 6;16(6):e61832. doi: 10.7759/cureus.61832. eCollection 2024 Jun. Cureus. 2024. PMID: 38975400 Free PMC article. Review.
Cited by
-
Application of spectral CT in diagnosis, classification and prognostic monitoring of gastrointestinal cancers: progress, limitations and prospects.Front Mol Biosci. 2023 Oct 25;10:1284549. doi: 10.3389/fmolb.2023.1284549. eCollection 2023. Front Mol Biosci. 2023. PMID: 37954980 Free PMC article. Review.
-
Dual-Energy Computed Tomography in Detecting and Predicting Lymph Node Metastasis in Malignant Tumor Patients: A Comprehensive Review.Diagnostics (Basel). 2024 Feb 9;14(4):377. doi: 10.3390/diagnostics14040377. Diagnostics (Basel). 2024. PMID: 38396416 Free PMC article. Review.
-
Impact of lymph node retrieval on prognosis in elderly and non-elderly patients with T3-4/N+ rectal cancer following neoadjuvant therapy: a retrospective cohort study.Int J Colorectal Dis. 2024 Jun 6;39(1):86. doi: 10.1007/s00384-024-04655-2. Int J Colorectal Dis. 2024. PMID: 38842538 Free PMC article.
-
Diagnosing cervical lymph node metastasis in oral squamous cell carcinoma based on third-generation dual-source, dual-energy computed tomography.Eur Radiol. 2023 Jan;33(1):162-171. doi: 10.1007/s00330-022-09033-6. Epub 2022 Sep 7. Eur Radiol. 2023. PMID: 36070090 Free PMC article.
-
Multi-DECT image-based radiomics with interpretable machine learning for preoperative prediction of tumor budding grade and prognosis in colorectal cancer: a dual-center study.Abdom Radiol (NY). 2025 Jul 16. doi: 10.1007/s00261-025-05112-6. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40668302
References
LinkOut - more resources
Full Text Sources