

Collaterals in portal hypertension: anatomy and clinical relevance
- PMID: 34341755
- PMCID: PMC8245950
- DOI: 10.21037/qims-20-1328
Collaterals in portal hypertension: anatomy and clinical relevance
Abstract
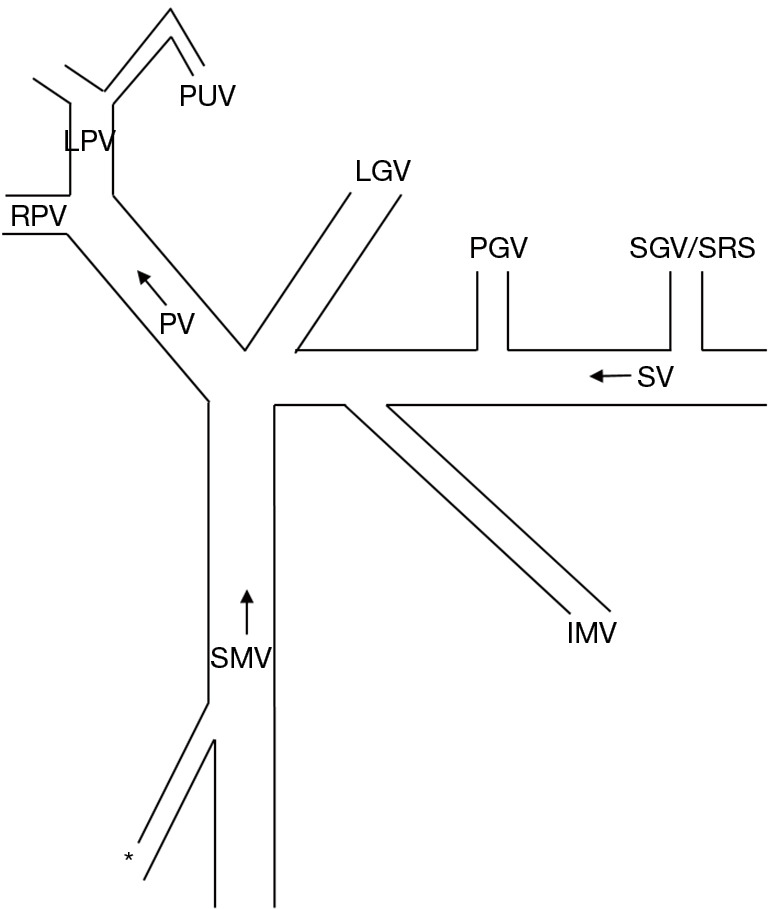
Portal hypertension is a key pathophysiology of chronic liver diseases typified with cirrhosis or noncirrhotic portal hypertension. The development of collateral vessels is a characteristic feature of impaired portal hemodynamics. The paraumbilical vein (PUV), left gastric vein (LGV), posterior gastric vein (PGV), short gastric vein (SGV), splenorenal shunt (SRS), and inferior mesenteric vein (IMV) are major collaterals, and there are some rare collaterals. The degree and hemodynamics of collateral may affect the portal venous circulation and may compensate for the balance between inflow and outflow volume of the liver. Additionally, the development of collateral shows a relation with the liver function reserve and clinical manifestations such as esophageal varices (EV), gastric varices, rectal varices and the other ectopic varices, hepatic encephalopathy, and prognosis. Furthermore, there may be an interrelationship in the development between different collaterals, showing additional influences on the clinical presentations. Thus, the assessment of collaterals may enhance the understanding of the underlying pathophysiology of the condition of patients with portal hypertension. This review article concluded that each collateral has a specific function depending on the anatomy and hemodynamics and is linked with the relative clinical presentation in patients with portal hypertension. Imaging modalities may be essential for the detection, grading and evaluation of the role of collaterals and may help to understand the pathophysiology of the patient condition. Further investigation in a large-scale study would elucidate the basic and clinical significance of collaterals in patients with portal hypertension and may provide information on how to manage them to improve the prognosis as well as quality of life.
Keywords: Doppler; Portal hypertension; cirrhosis; collateral; ectopic varices; esophageal varices (EV); gastric varices; hepatic encephalopathy; hepatic venous pressure gradient (HVPG); shunt; ultrasound (US).
2021 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: Both authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/qims-20-1328). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
64-row multidetector computed tomography portal venography of gastric variceal collateral circulation.World J Gastroenterol. 2010 Feb 28;16(8):1003-7. doi: 10.3748/wjg.v16.i8.1003. World J Gastroenterol. 2010. PMID: 20180241 Free PMC article.
-
Portosystemic shunts in a large cohort of patients with liver cirrhosis: detection rate and clinical relevance.J Gastroenterol. 2009;44(1):76-83. doi: 10.1007/s00535-008-2279-1. Epub 2009 Jan 22. J Gastroenterol. 2009. PMID: 19159076
-
Interrelationship between insulin resistance and portal haemodynamic abnormality in cirrhosis.Int J Med Sci. 2017 Feb 23;14(3):240-245. doi: 10.7150/ijms.17738. eCollection 2017. Int J Med Sci. 2017. PMID: 28367084 Free PMC article.
-
Collateral pathways in portal hypertension.J Clin Exp Hepatol. 2012 Dec;2(4):338-52. doi: 10.1016/j.jceh.2012.08.001. Epub 2012 Dec 16. J Clin Exp Hepatol. 2012. PMID: 25755456 Free PMC article. Review.
-
Color Doppler Ultrasound in Portal Hypertension: A Closer Look at Left Gastric Vein Hemodynamics.J Ultrasound Med. 2021 Jan;40(1):7-14. doi: 10.1002/jum.15386. Epub 2020 Jul 13. J Ultrasound Med. 2021. PMID: 32657462 Review.
Cited by
-
Non-contrast-enhanced MR angiography of left gastric vein in patients with gastroesophageal varices: morphology and blood supply analysis.Eur Radiol. 2024 Jul;34(7):4686-4696. doi: 10.1007/s00330-023-10497-3. Epub 2023 Dec 22. Eur Radiol. 2024. PMID: 38133674
-
Portal hypertensive enteropathy: multimodality assessment through computed tomography and magnetic resonance enterography.Radiol Case Rep. 2022 Oct 5;17(12):4804-4808. doi: 10.1016/j.radcr.2022.09.046. eCollection 2022 Dec. Radiol Case Rep. 2022. PMID: 36212766 Free PMC article.
-
Predictive value of blood coagulation and routine blood indices for rebleeding after endoscopic treatment in hepatitis B-related cirrhotic patients with esophagogastric fundal varices: a logistic regression model analysis.Am J Transl Res. 2024 Jul 15;16(7):2982-2994. doi: 10.62347/ICQU1086. eCollection 2024. Am J Transl Res. 2024. PMID: 39114728 Free PMC article.
-
Case of Ectopic Variceal Bleed Managed With Percutaneous Transhepatic Portal Vein Recanalization.J Clin Exp Hepatol. 2024 Sep-Oct;14(5):101429. doi: 10.1016/j.jceh.2024.101429. Epub 2024 Apr 16. J Clin Exp Hepatol. 2024. PMID: 38766622
-
Interorgan communication with the liver: novel mechanisms and therapeutic targets.Front Immunol. 2023 Dec 12;14:1314123. doi: 10.3389/fimmu.2023.1314123. eCollection 2023. Front Immunol. 2023. PMID: 38155961 Free PMC article. Review.
References
-
- WHO Global hepatitis report 2017. Geneva: World Health Organization, 2017.
Publication types
LinkOut - more resources
Full Text Sources