

A novel use of biomechanical model-based deformable image registration (DIR) for assessing colorectal liver metastases ablation outcomes
- PMID: 34342018
- PMCID: PMC9380122
- DOI: 10.1002/mp.15147
A novel use of biomechanical model-based deformable image registration (DIR) for assessing colorectal liver metastases ablation outcomes
Abstract
Purpose: Colorectal cancer is the third most common form of cancer in the United States, and up to 60% of these patients develop liver metastasis. While hepatic resection is the curative treatment of choice, only 20% of patients are candidates at the time of diagnosis. While percutaneous thermal ablation (PTA) has demonstrated 24%-51% overall 5-year survival rates, assurance of sufficient ablation margin delivery (5 mm) can be challenging, with current methods of 2D distance measurement not ensuring 3D minimum margin. We hypothesized that biomechanical model-based deformable image registration (DIR) can reduce spatial uncertainties and differentiate local tumor progression (LTP) patients from LTP-free patients.
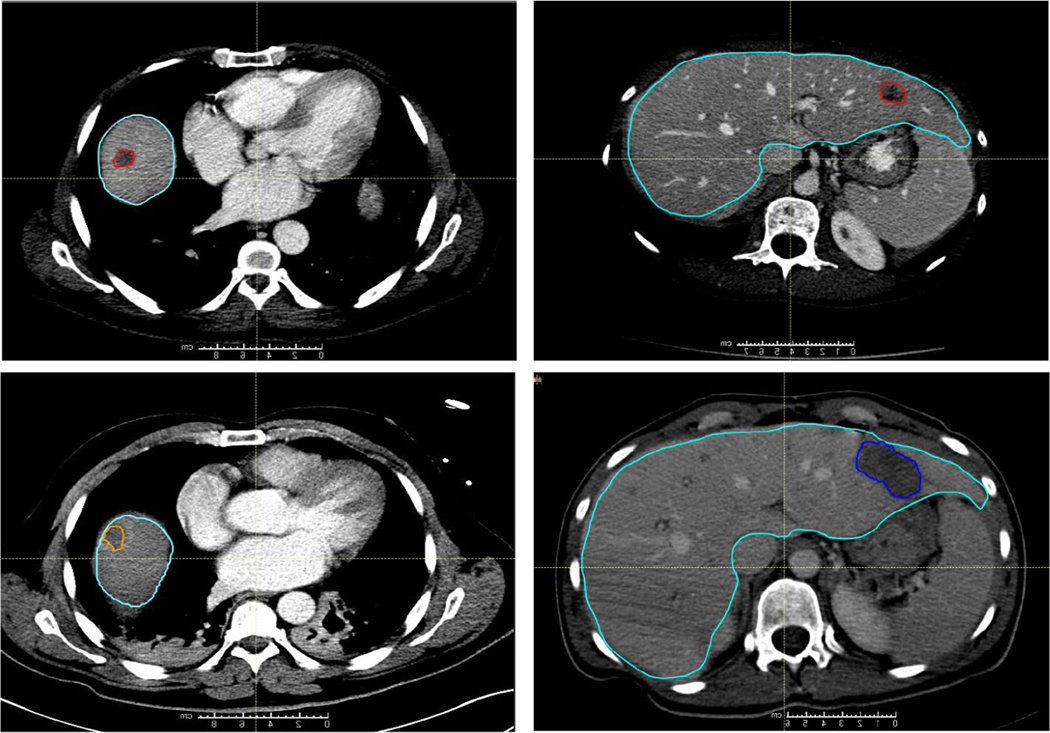
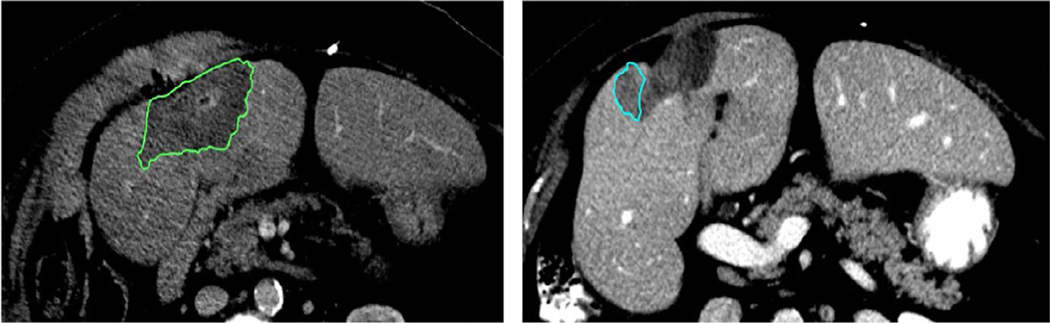
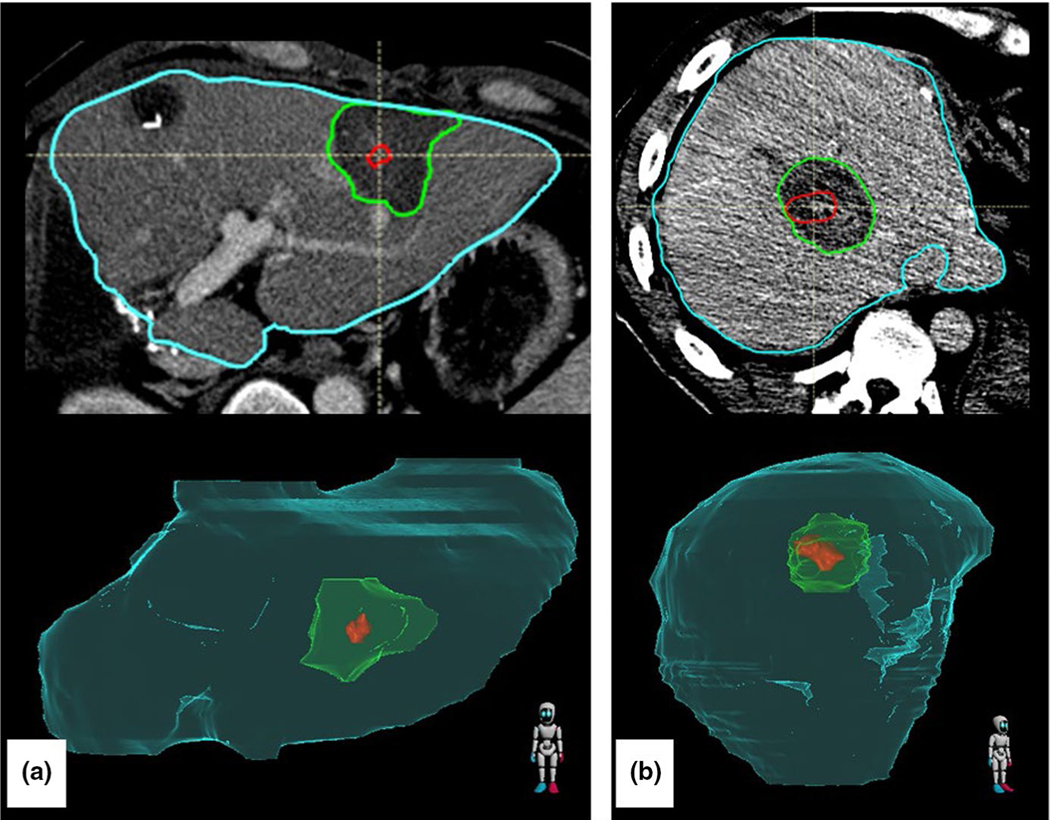
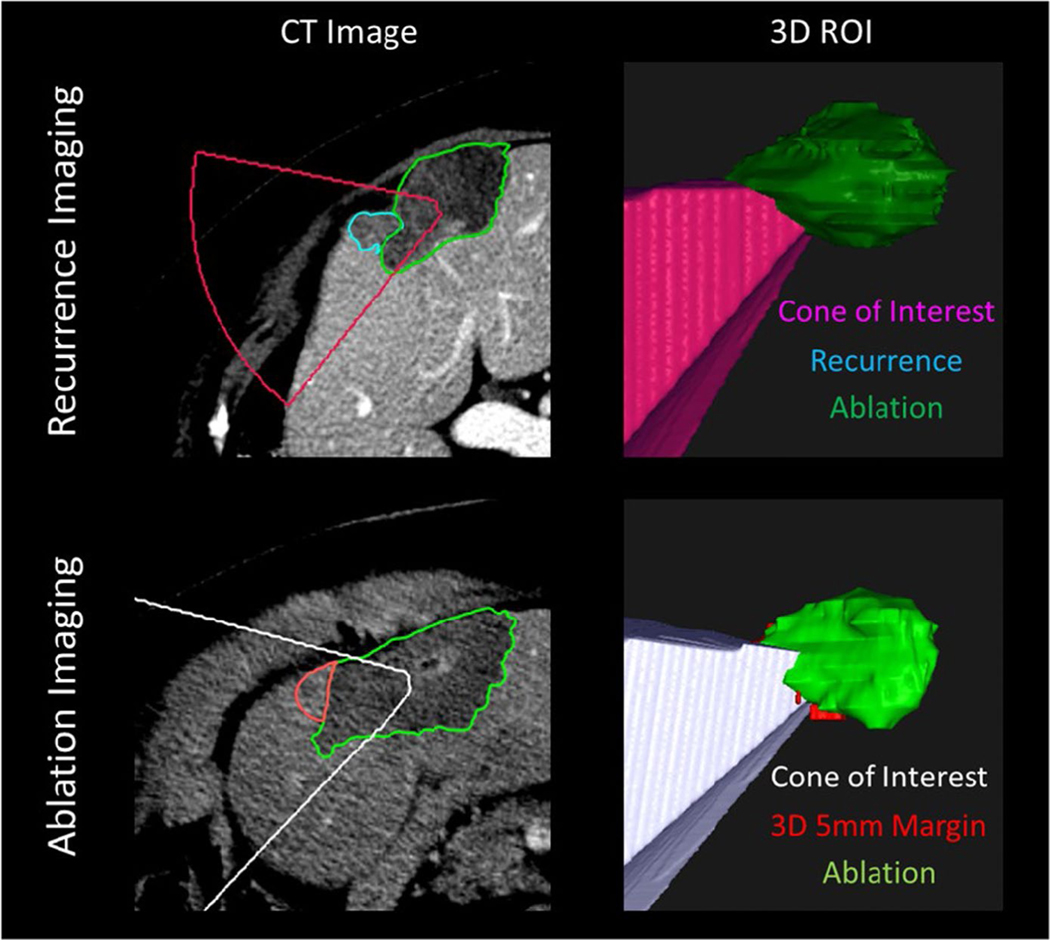
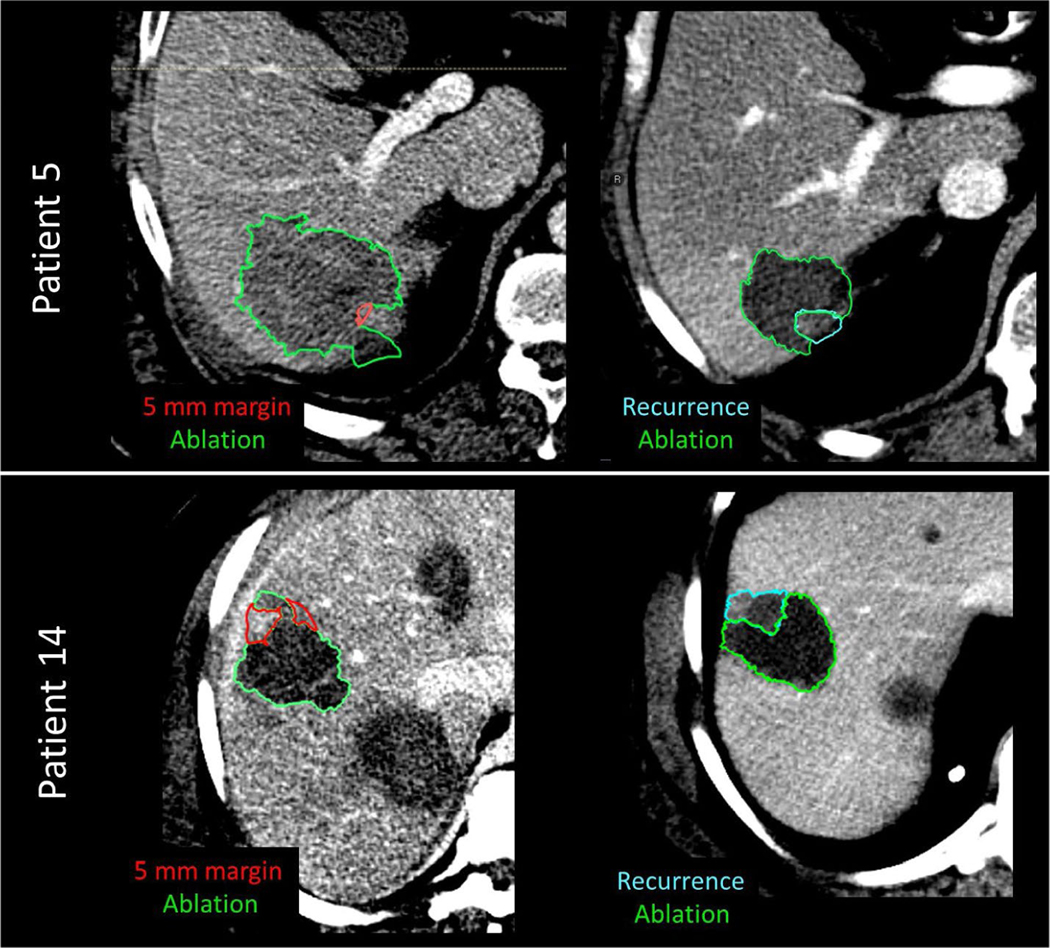
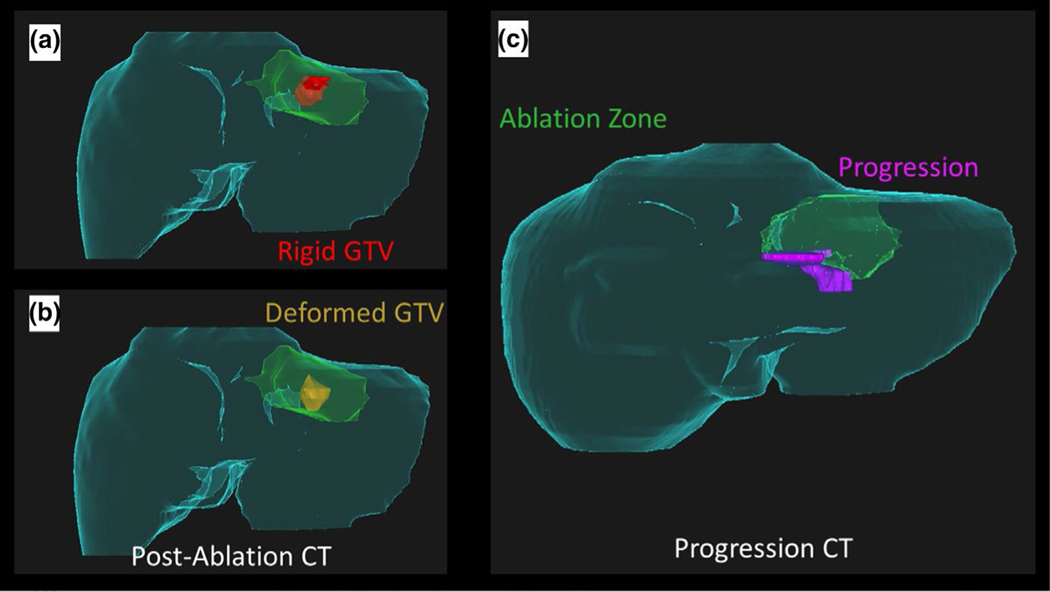
Methods: We retrospectively acquired 30 patients (16 LTP and 14 LTP-free) at our institution who had undergone PTA and had a contrast-enhanced pre-treatment and post-ablation CT scan. Liver, disease, and ablation zone were manually segmented. Biomechanical model-based DIR between the pre-treatment and post-ablation CT mapped the gross tumor volume onto the ablation zone and measured 3D minimum delivered margin (MDM). An in-house cone-tracing algorithm determined if progression qualitatively collocated with insufficient 5 mm margin achieved.
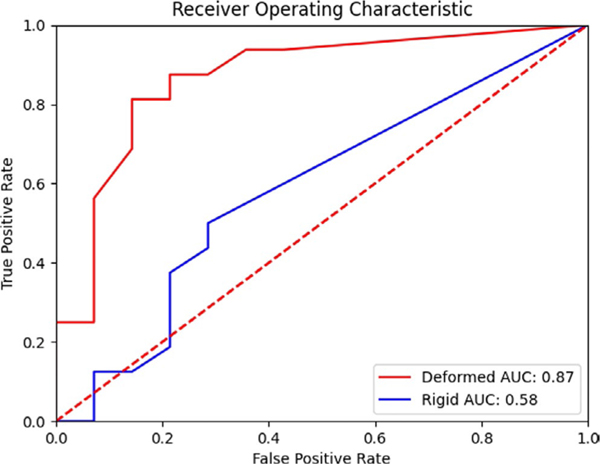
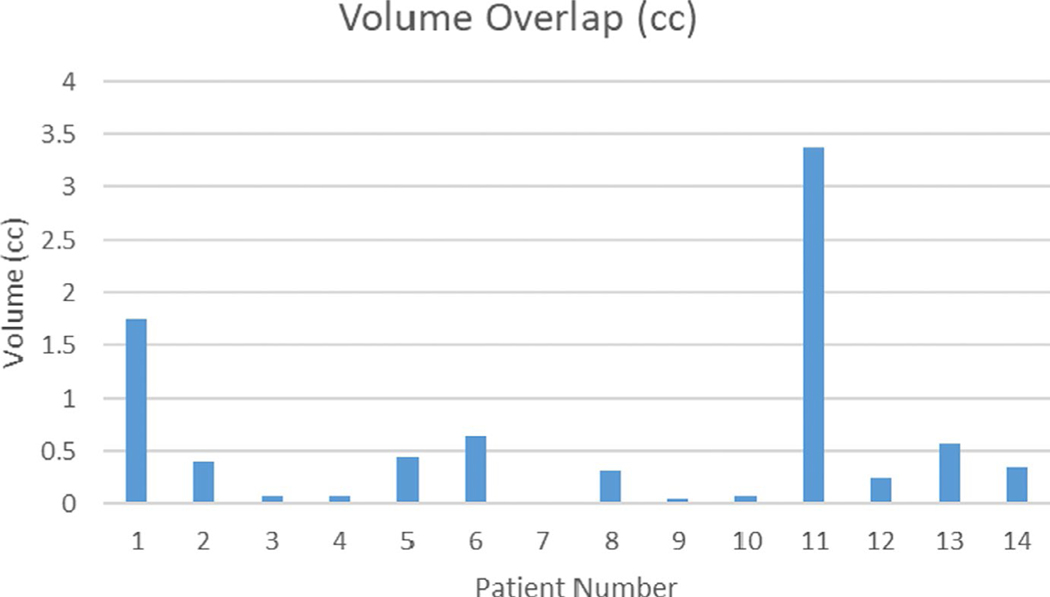
Results: Mann-Whitney U test showed a significant difference (p < 0.01) in MDM from the LTP and LTP-free groups. A total of 93% (13/14) of patients with LTP had a correlation between progression and missing 5 mm of margin volume.
Conclusions: Biomechanical DIR is able to reduce spatial uncertainty and allow measurement of delivered 3D MDM. This minimum margin can help ensure sufficient ablation delivery, and our workflow can provide valuable information in a clinically useful timeframe.
Keywords: biomechanical model-based deformable image registration; colorectal cancer; colorectal liver metastases; liver ablation therapy.
© 2021 American Association of Physicists in Medicine.
Conflict of interest statement
CONFLICT OF INTEREST
Dr. Brock reports grants from National Institutes of Health R01CA235564, R01CA221971, during the conduct of the study; grants from RaySearch Laboratories, outside the submitted work. Dr. Cazoulat reports grants from NIH, during the conduct of the study; grants from RaySearch Laboratories, outside the submitted work. Dr. Odisio reports grants from NIH, grants from Society of Interventional Radiology, during the conduct of the study. Dr. Bruno Odisio received grants from Siemens Healthineers and other incentives from Koo Foundation outside of the submitted work.
Figures
References
-
- WHO Biennial Report 2012–2013. Accessed October 27, 2020. https://governance.iarc.fr/SC/SC50/BiennialReport2012-2013.pdf
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
