

Association of Dose Tapering With Overdose or Mental Health Crisis Among Patients Prescribed Long-term Opioids
- PMID: 34342618
- PMCID: PMC8335575
- DOI: 10.1001/jama.2021.11013
Association of Dose Tapering With Overdose or Mental Health Crisis Among Patients Prescribed Long-term Opioids
Erratum in
-
Cancer Line.JAMA. 2022 Feb 15;327(7):688. doi: 10.1001/jama.2021.22379. JAMA. 2022. PMID: 35166798 No abstract available.
-
Errors in Data Analysis and Outcomes Coding.JAMA. 2022 Feb 15;327(7):687. doi: 10.1001/jama.2022.0231. JAMA. 2022. PMID: 35166820 Free PMC article. No abstract available.
Abstract
Importance: Opioid-related mortality and national prescribing guidelines have led to tapering of doses among patients prescribed long-term opioid therapy for chronic pain. There is limited information about risks related to tapering, including overdose and mental health crisis.
Objective: To assess whether there are associations between opioid dose tapering and rates of overdose and mental health crisis among patients prescribed stable, long-term, higher-dose opioids.
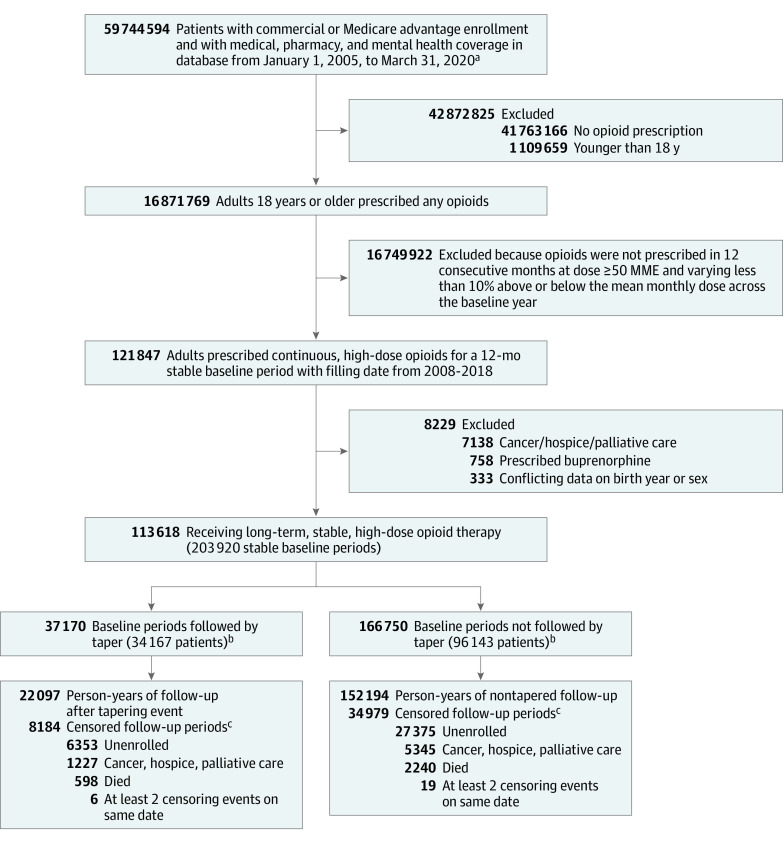
Design, setting, and participants: Retrospective cohort study using deidentified medical and pharmacy claims and enrollment data from the OptumLabs Data Warehouse from 2008 to 2019. Adults in the US prescribed stable higher doses (mean ≥50 morphine milligram equivalents/d) of opioids for a 12-month baseline period with at least 2 months of follow-up were eligible for inclusion.
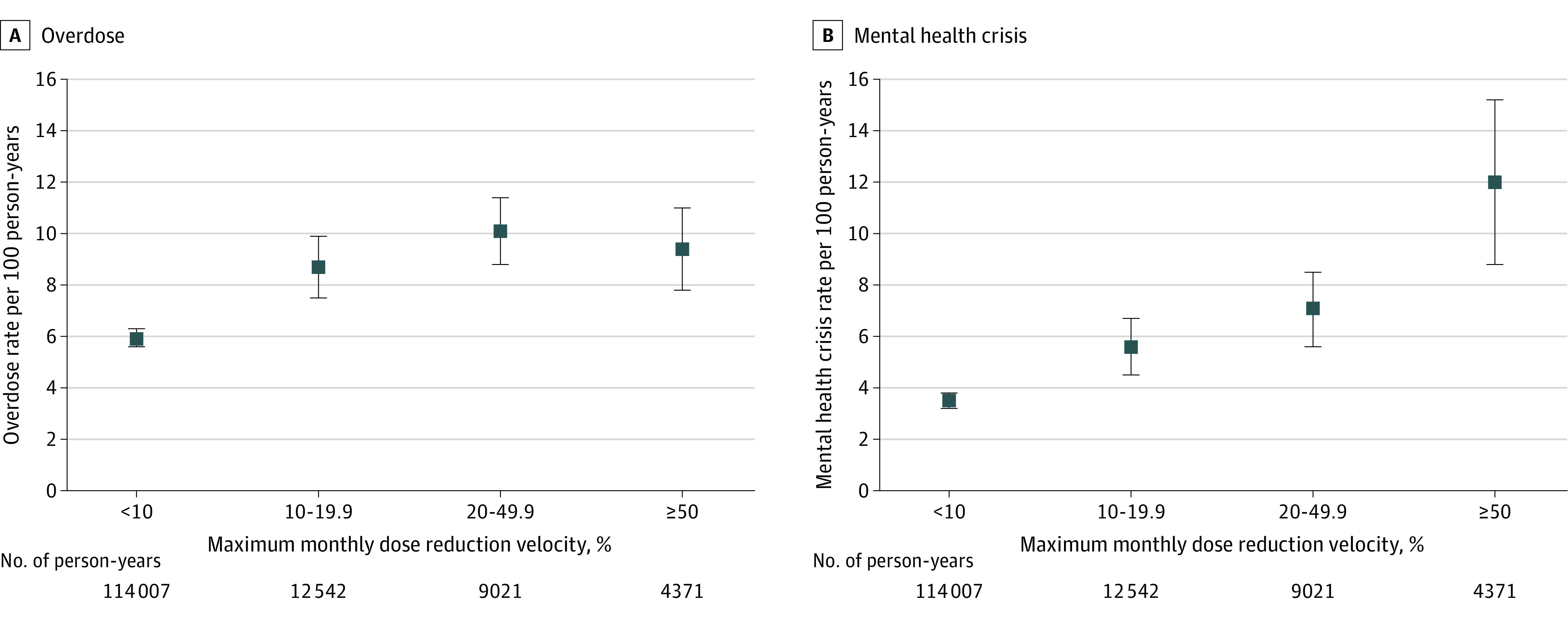
Exposures: Opioid tapering, defined as at least 15% relative reduction in mean daily dose during any of 6 overlapping 60-day windows within a 7-month follow-up period. Maximum monthly dose reduction velocity was computed during the same period.
Main outcomes and measures: Emergency or hospital encounters for (1) drug overdose or withdrawal and (2) mental health crisis (depression, anxiety, suicide attempt) during up to 12 months of follow-up. Discrete time negative binomial regression models estimated adjusted incidence rate ratios (aIRRs) of outcomes as a function of tapering (vs no tapering) and dose reduction velocity.
Results: The final cohort included 113 618 patients after 203 920 stable baseline periods. Among the patients who underwent dose tapering, 54.3% were women (vs 53.2% among those who did not undergo dose tapering), the mean age was 57.7 years (vs 58.3 years), and 38.8% were commercially insured (vs 41.9%). Posttapering patient periods were associated with an adjusted incidence rate of 9.3 overdose events per 100 person-years compared with 5.5 events per 100 person-years in nontapered periods (adjusted incidence rate difference, 3.8 per 100 person-years [95% CI, 3.0-4.6]; aIRR, 1.68 [95% CI, 1.53-1.85]). Tapering was associated with an adjusted incidence rate of 7.6 mental health crisis events per 100 person-years compared with 3.3 events per 100 person-years among nontapered periods (adjusted incidence rate difference, 4.3 per 100 person-years [95% CI, 3.2-5.3]; aIRR, 2.28 [95% CI, 1.96-2.65]). Increasing maximum monthly dose reduction velocity by 10% was associated with an aIRR of 1.09 for overdose (95% CI, 1.07-1.11) and of 1.18 for mental health crisis (95% CI, 1.14-1.21).
Conclusions and relevance: Among patients prescribed stable, long-term, higher-dose opioid therapy, tapering events were significantly associated with increased risk of overdose and mental health crisis. Although these findings raise questions about potential harms of tapering, interpretation is limited by the observational study design.
Conflict of interest statement
Figures
Comment in
-
Opioid Tapering Practices-Time for Reconsideration?JAMA. 2021 Aug 3;326(5):388-389. doi: 10.1001/jama.2021.11118. JAMA. 2021. PMID: 34342635 No abstract available.
-
In long-term, higher-dose opioid use, dose tapering was linked to overdose and mental health crises.Ann Intern Med. 2022 Jan;175(1):JC11. doi: 10.7326/J21-0005. Epub 2022 Jan 4. Ann Intern Med. 2022. PMID: 34978849
-
Errors in Data Analysis and Outcomes Coding in Study of Dose Tapering and Overdose or Mental Health Crisis in Patients Prescribed Opioids.JAMA. 2022 Feb 15;327(7):687. doi: 10.1001/jama.2022.0323. JAMA. 2022. PMID: 35166803 No abstract available.
