

Effect of a Sedation and Ventilator Liberation Protocol vs Usual Care on Duration of Invasive Mechanical Ventilation in Pediatric Intensive Care Units: A Randomized Clinical Trial
- PMID: 34342620
- PMCID: PMC8335576
- DOI: 10.1001/jama.2021.10296
Effect of a Sedation and Ventilator Liberation Protocol vs Usual Care on Duration of Invasive Mechanical Ventilation in Pediatric Intensive Care Units: A Randomized Clinical Trial
Abstract
Importance: There is limited evidence on the optimal strategy for liberating infants and children from invasive mechanical ventilation in the pediatric intensive care unit.
Objective: To determine if a sedation and ventilator liberation protocol intervention reduces the duration of invasive mechanical ventilation in infants and children anticipated to require prolonged mechanical ventilation.
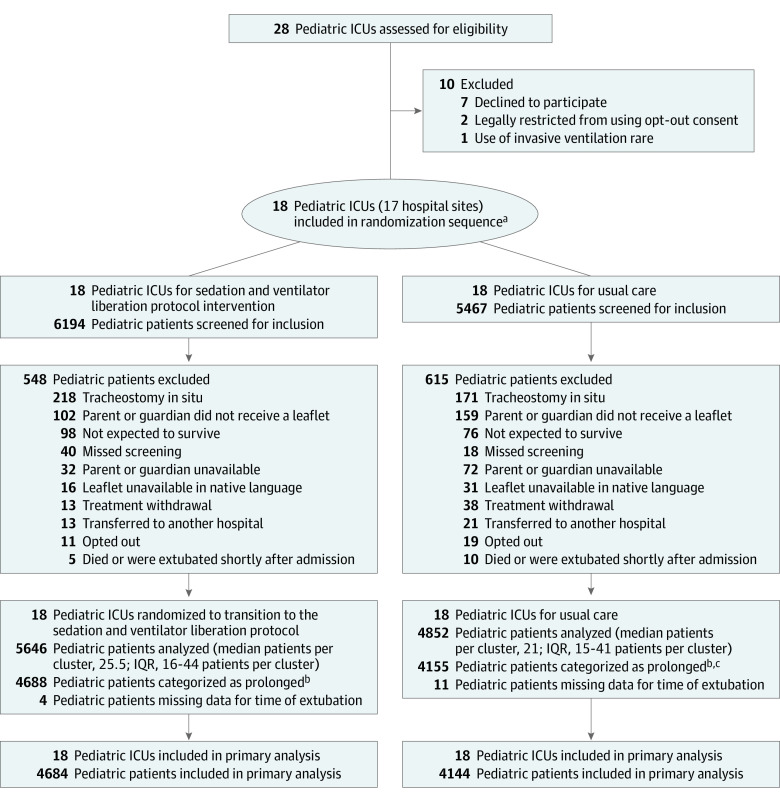
Design, setting, and participants: A pragmatic multicenter, stepped-wedge, cluster randomized clinical trial was conducted that included 17 hospital sites (18 pediatric intensive care units) in the UK sequentially randomized from usual care to the protocol intervention. From February 2018 to October 2019, 8843 critically ill infants and children anticipated to require prolonged mechanical ventilation were recruited. The last date of follow-up was November 11, 2019.
Interventions: Pediatric intensive care units provided usual care (n = 4155 infants and children) or a sedation and ventilator liberation protocol intervention (n = 4688 infants and children) that consisted of assessment of sedation level, daily screening for readiness to undertake a spontaneous breathing trial, a spontaneous breathing trial to test ventilator liberation potential, and daily rounds to review sedation and readiness screening and set patient-relevant targets.
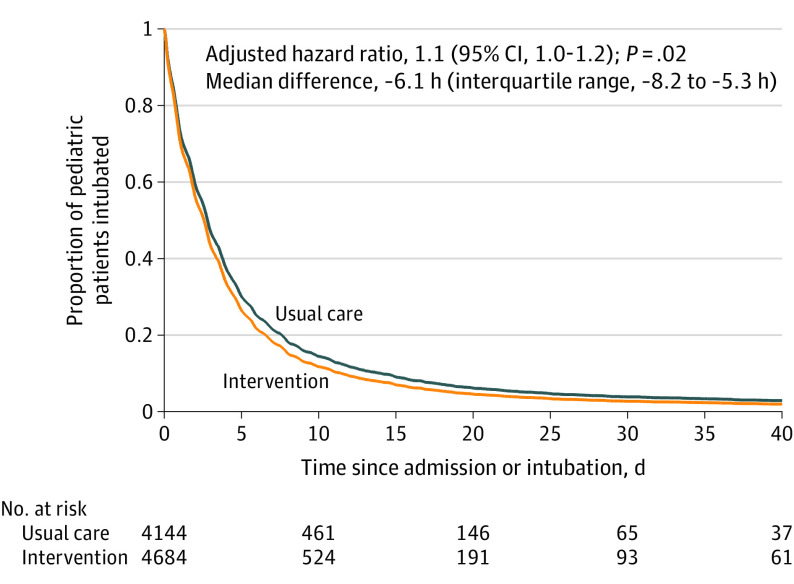
Main outcomes and measures: The primary outcome was the duration of invasive mechanical ventilation from initiation of ventilation until the first successful extubation. The primary estimate of the treatment effect was a hazard ratio (with a 95% CI) adjusted for calendar time and cluster (hospital site) for infants and children anticipated to require prolonged mechanical ventilation.
Results: There were a total of 8843 infants and children (median age, 8 months [interquartile range, 1 to 46 months]; 42% were female) who completed the trial. There was a significantly shorter median time to successful extubation for the protocol intervention compared with usual care (64.8 hours vs 66.2 hours, respectively; adjusted median difference, -6.1 hours [interquartile range, -8.2 to -5.3 hours]; adjusted hazard ratio, 1.11 [95% CI, 1.02 to 1.20], P = .02). The serious adverse event of hypoxia occurred in 9 (0.2%) infants and children for the protocol intervention vs 11 (0.3%) for usual care; nonvascular device dislodgement occurred in 2 (0.04%) vs 7 (0.1%), respectively.
Conclusions and relevance: Among infants and children anticipated to require prolonged mechanical ventilation, a sedation and ventilator liberation protocol intervention compared with usual care resulted in a statistically significant reduction in time to first successful extubation. However, the clinical importance of the effect size is uncertain.
Trial registration: isrctn.org Identifier: ISRCTN16998143.
Conflict of interest statement
Figures
Comment in
-
Sedation and Ventilator Liberation Protocol vs Usual Care and Duration of Invasive Ventilation in Pediatric Intensive Care Units.JAMA. 2021 Dec 14;326(22):2328-2329. doi: 10.1001/jama.2021.17728. JAMA. 2021. PMID: 34905039 No abstract available.
-
What's new in paediatric ventilator liberation?Intensive Care Med. 2022 Nov;48(11):1635-1637. doi: 10.1007/s00134-022-06865-0. Epub 2022 Sep 1. Intensive Care Med. 2022. PMID: 36048243 No abstract available.
References
-
- Balcells Ramírez J, López-Herce Cid J, Modesto Alapont V; Grupo de Respiratorio de la Sociedad Española de Cuidados Intensivos Pediátricos . Prevalence of mechanical ventilation in pediatric intensive care units in Spain. Published in Spanish. An Pediatr (Barc). 2004;61(6):533-541. - PubMed
-
- Farias JA, Fernández A, Monteverde E, et al. ; Latin-American Group for Mechanical Ventilation in Children . Mechanical ventilation in pediatric intensive care units during the season for acute lower respiratory infection: a multicenter study. Pediatr Crit Care Med. 2012;13(2):158-164. doi: 10.1097/PCC.0b013e3182257b82 - DOI - PubMed
-
- Paediatric Intensive Care Audit Network . 2019 annual report. Accessed July 16, 2020. https://www.picanet.org.uk/annual-reporting-and-publications/
-
- Curley MA, Wypij D, Watson RS, et al. ; RESTORE Study Investigators and the Pediatric Acute Lung Injury and Sepsis Investigators Network . Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: a randomized clinical trial. JAMA. 2015;313(4):379-389. doi: 10.1001/jama.2014.18399 - DOI - PMC - PubMed
